
A new report on Covid reinfections is quite concerning. It’s currently a preprint but these same authors with access to the US largest healthcare system, the Veteran Affairs, have published numerous eye-opening studies during the pandemic, in leading peer-review journals, on topics which include Long Covid cardiovascular outcomes, diabetes, breakthrough infections, the toll on mental health, and kidney disease. I have not previously seen any substantive differences from their preprints compared with the final publications. So with that context let’s look at their findings from >250,000 people with 1 infection, ~39,000 people with 2 or more infections, and nearly 5.4 million uninfected controls. It’s the first study to characterize the risks of reinfection.
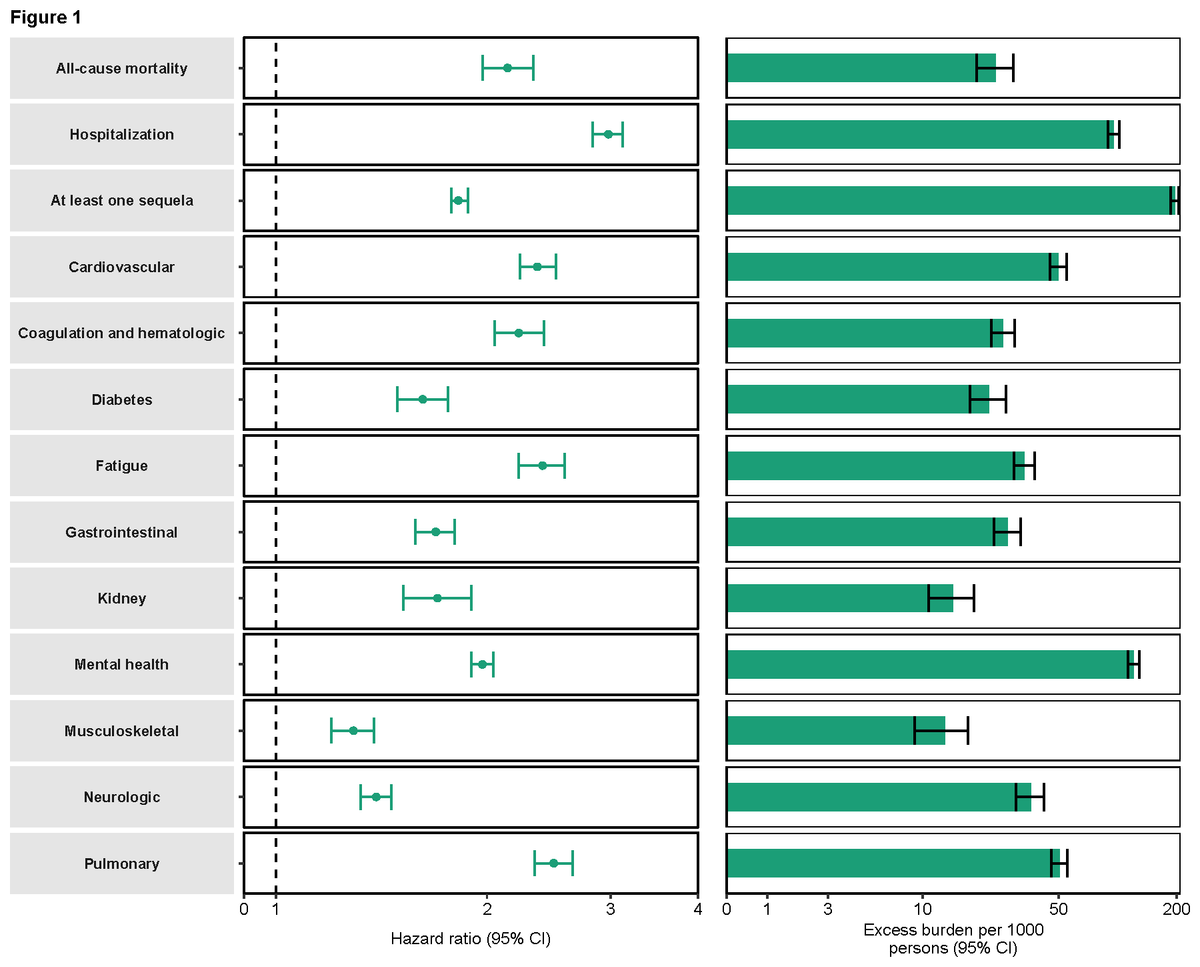
The first finding is the comparison of people with reinfections vs those with only 1 infection. Note the doubling of all-cause mortality, cardiovascular, and lung adverse outcomes, 3-fold risk of hospitalization, and impact on other health domains. The absolute excess burden is shown on the right panel.
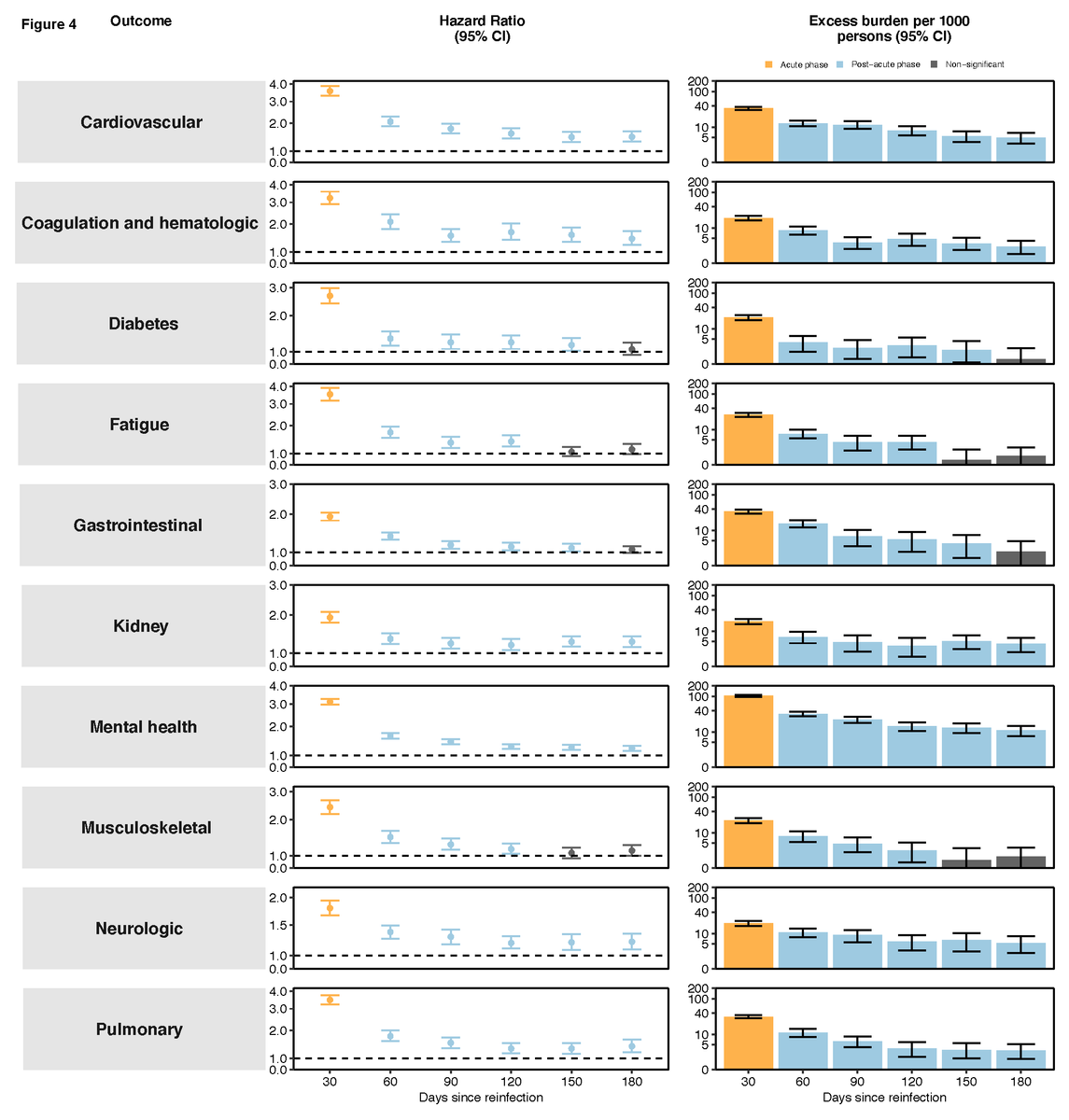
Next is the durability of these adverse outcomes for this same comparison (reinfections vs 1 infection) in 30-day increments, indicating that much of the hit was up front, but persistent increased risk was evident for most endpoints throughout the 6 months follow-up (above the line of 1.0, hazard ratio, in the left hand panel).
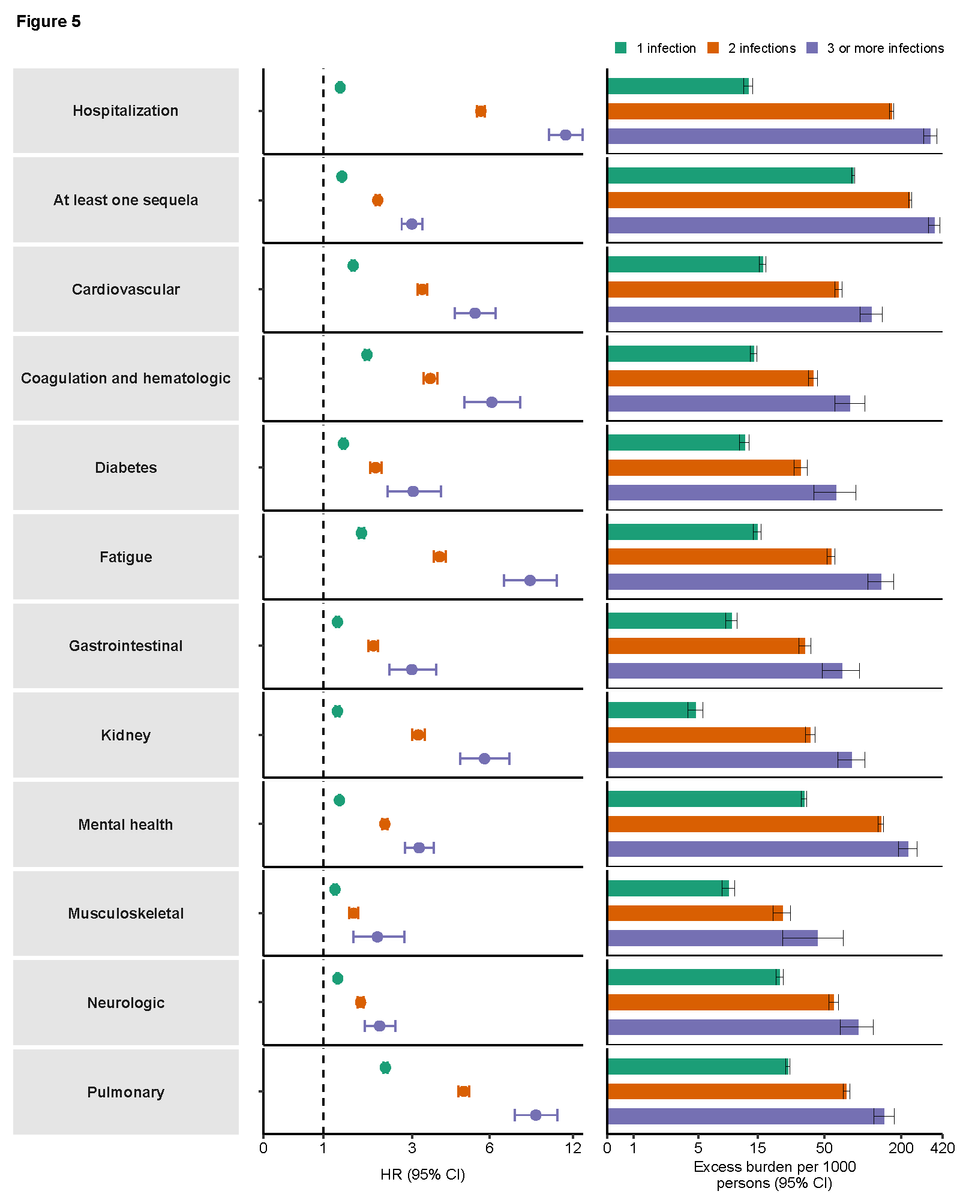
Finally, there is the “dose-response” effect of multiple reinfections. By that I mean with additional episodes of Covid, for every outcome there was a stepwise increased risk, both relative (left panel) and absolute (right panel).
Obviously these findings are worrisome since reinfection was quite rare before the Omicron wave hit, at 1% or less through the Delta variant wave. But now reinfections have become much more common. Why? The Omicron BA.2, BA.2.12.1, BA.4, and BA.5 have progressively increased immune escape and there is limited cross-immunity with BA.1, the Omicron version that about half of Americans got infected with early in 2022. We await an independent replication of these reinfection findings, but I note much of what these authors have thus far published from the Veterans Affairs information resource has indeed been replicated.
The new Omicron subvariants portend much more reinfections
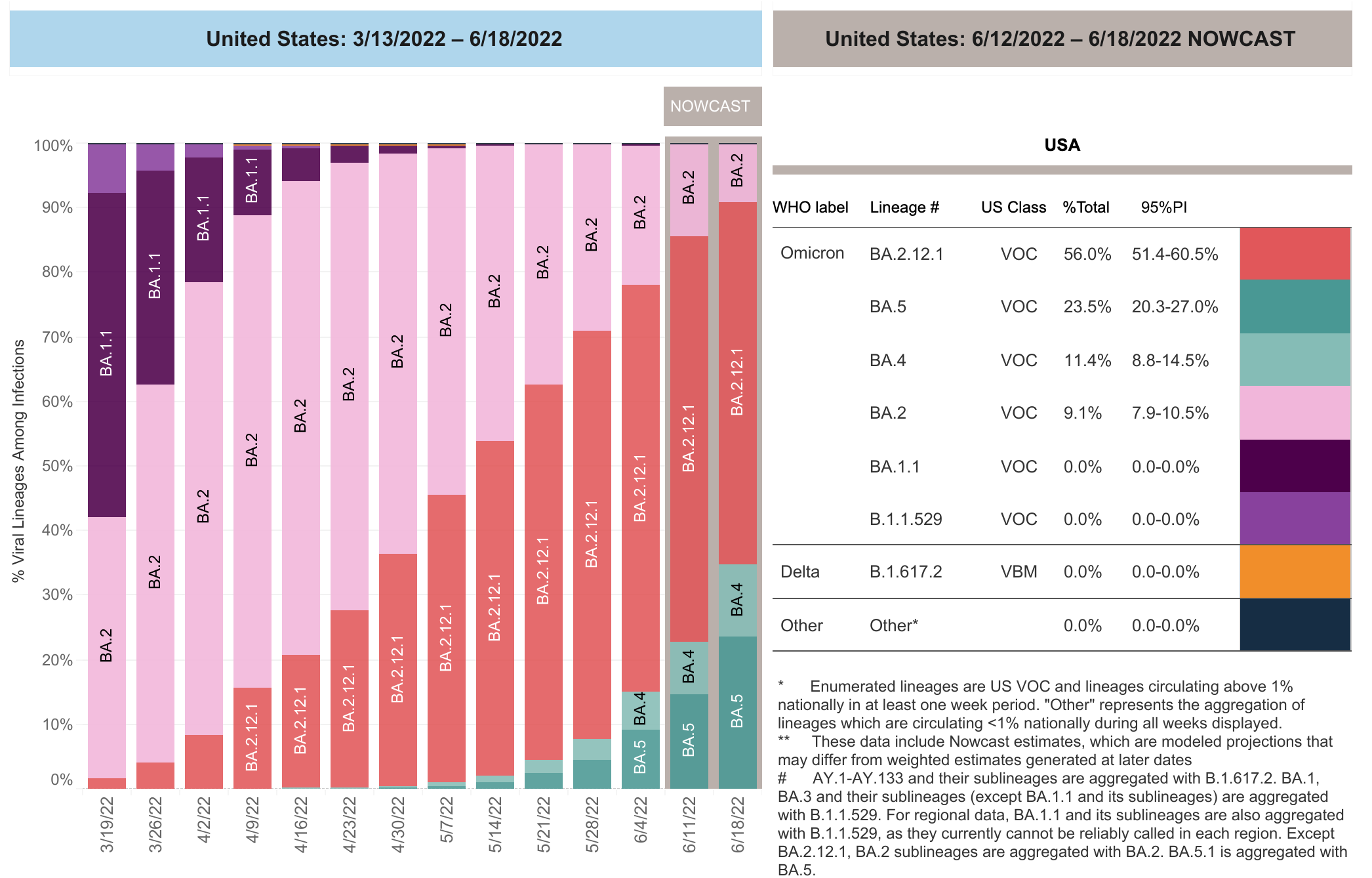
Today’s CDC update of genomics shows we have 35% of new cases accounted by the BA.4/5 variants, which have the most immune-evasiveness of any variant since the pandemic began, and 56% by BA.2.12.1.
Reinfection risk is substantially increased due to the new spike mutations we are getting exposed to, as simplified below. BA.2.12.1 presented the L452Q mutation and BA.4/5 add 2 other key mutations. BA.1 induces a fairly weak, narrow immune response which doesn’t help with exposure to the BA.2.12.1 and BA.4/5 subvaraints.
We’re not alone in facing a new BA.4/5 wave, which we saw initially in South Africa and Portugal, but now is occurring in the UK, many countries in Europe and Australia, with at least some increase in hospitalizations associated with these subvariants
Although we just saw a favorable report about less 50-70% less Long Covid with Omicron compared with Delta, remember the number of infections with Omicron and its subvariants is markedly higher than any previous wave, including Delta, such that the absolute risk of developing Long Covid is still real, no less the burden at the population level.
The Omicron BA.1-specific vaccine booster remedy?
The worry is centered about the immune escape of these subvariants, which was characterized in a recent Nature paper with the conclusion “Together, our results indicate that Omicron may evolve mutations to evade the humoral immunity elicited by BA.1 infection, suggesting that BA.1-derived vaccine boosters may not achieve broad-spectrum protection against new Omicron variants.” That is to say, besides vulnerability to reinfections, the Omicron BA.1 specific vaccines, due to become available this Fall, may not provide enhanced protection as anticipated. BA.4/5 are too different from BA.1 with respect to how our immune system sees them. Even the head of BioNTech has recently warned about the potential for further immune escape and the reduced impact of vaccines, including an Omicron-BA.1 specific one.
We are already seeing evidence of some less protection against severe Covid, that requiring hospitalization, with recent reports of vaccine effectiveness, such as 77% in 21 United States hospitals among immunocompetent individuals with 3 shots. Recall the mRNA vaccine effectiveness vs. hospitalization was 95% through Delta. We don’t have adequate data for vaccine protection vs BA.4/5 yet, but it is certainly possible there will be some attrition which has fortunately not been noted between BA.1 and BA.2.
What should we do about this?
Despite lack of warnings by CDC, there should be gearing up with N95/KN95 masks, distancing when possible, attention to ventilation, air filtration, and all of the non-pharmacologic measures that we have at our disposal to limit infections and reinfections.
Booster shots can help, especially when more than 4 months have elapsed from primary vaccination or a third shot. Children of all ages will benefit from vaccination, including the new approval for age < 5 years, even if they have had Omicron infections with BA.1, owing to the narrow and often insufficient immune response that may not protect from BA.4/5 and subsequent variants.
Beyond that is my #1 frustration as expressed here.
There is simply no excuse for why these vaccines are not being hyper-aggressively pursued, particularly given the trajectory of relentless increased SARS-CoV-2 immune-evasiveness (and resultant enhanced transmissibility), the new worry about reinfection sequelae and Long Covid, and the known unknown next Greek letter variant we may well be seeing in the months ahead. The lack of priority and resource allocation stems from the illusion that the pandemic is behind us, which is obviously off-base. If ever there was a callout for don’t just stand there, do something, this is it.