


Covid, 4 years on
A quick update on some important new data
As we recently hit—March 11, 2020—the 4-year anniversary of when WHO finally declared Covid a global pandemic, and today, March 13th, when the US declared it a national emergency, we’re still learning every day about SARS-CoV-2’s impact, its evolution, protection from vaccination, and more. Here’s a quick summary of what I think is worth reviewing:
Impact
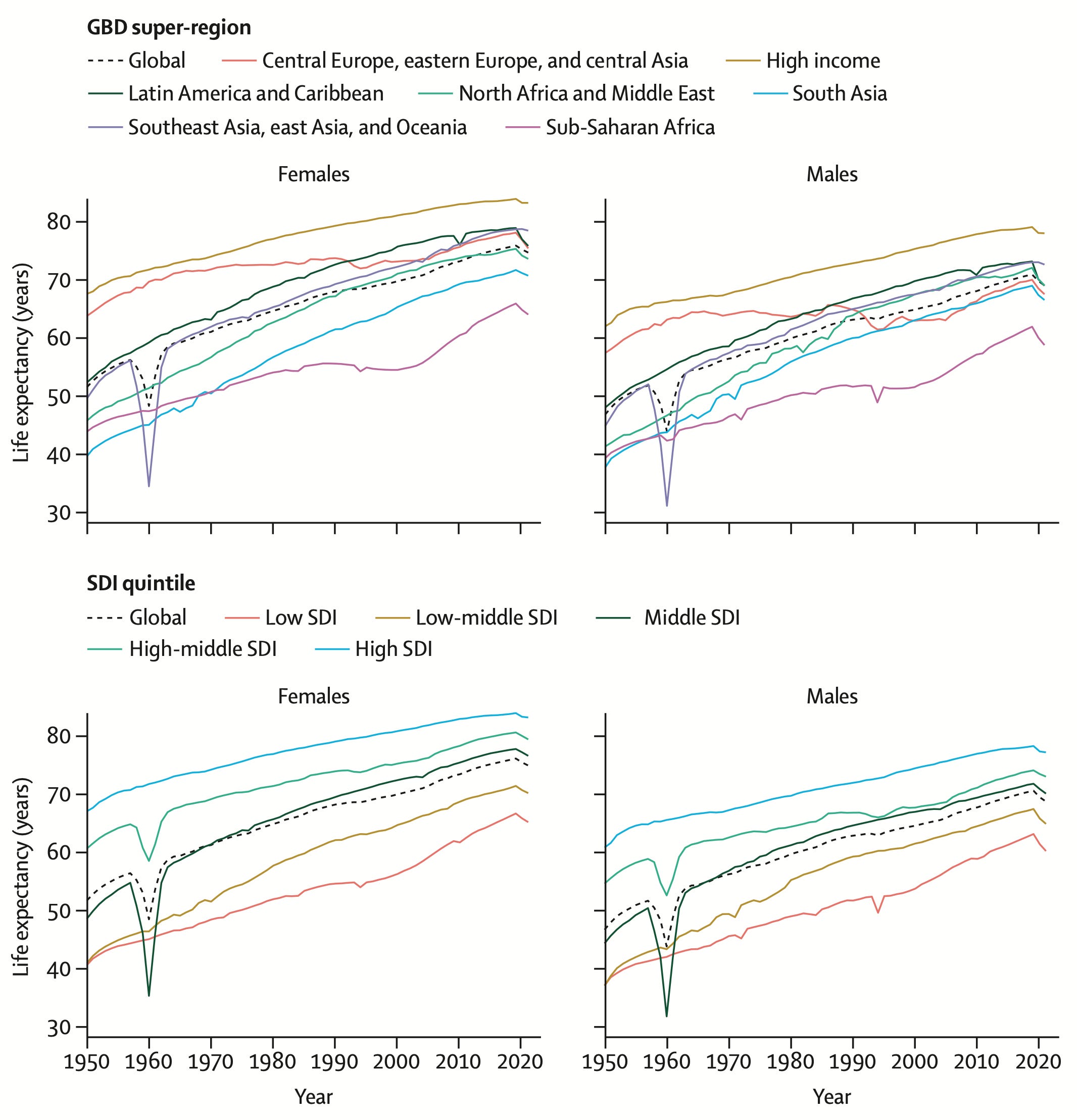
The global excess mortality has reached about 30 million lost lives attributable to Covid, and the Global Burden of Disease published a major paper this week in The Lancet on the toll it has taken for reducing life expectancy in 204 countries summarized as "The COVID-19 pandemic caused the most severe drops in life expectancy seen in 50+ years." The study did not address disability among survivors, with multiple concurrent studies reinforcing the prevalence of Long Covid in tens of millions of people.
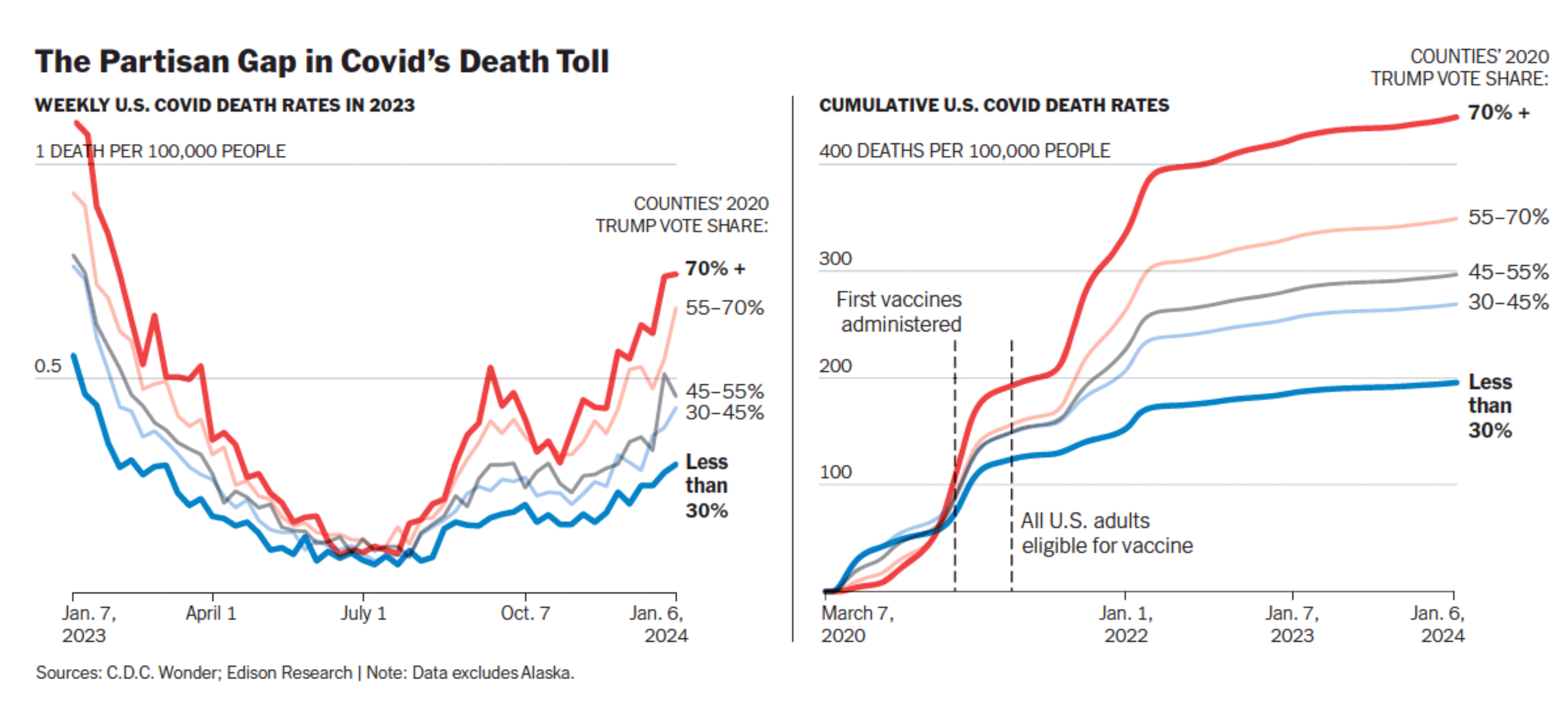
Here in the United States, it is striking to review the updated data on partisan gap death rates, as reflected by counties who voted Republican in the 2020 election. As you can see below from Ashley Wu, graphics editor at the New York Times, the curves are continuing to diverge, both weekly and cumulatively. There was no divergence when vaccines were first administered (right panel below) but since that time the death rates continue to worsen in counties with 70%+ Republican voters compared with <30%.
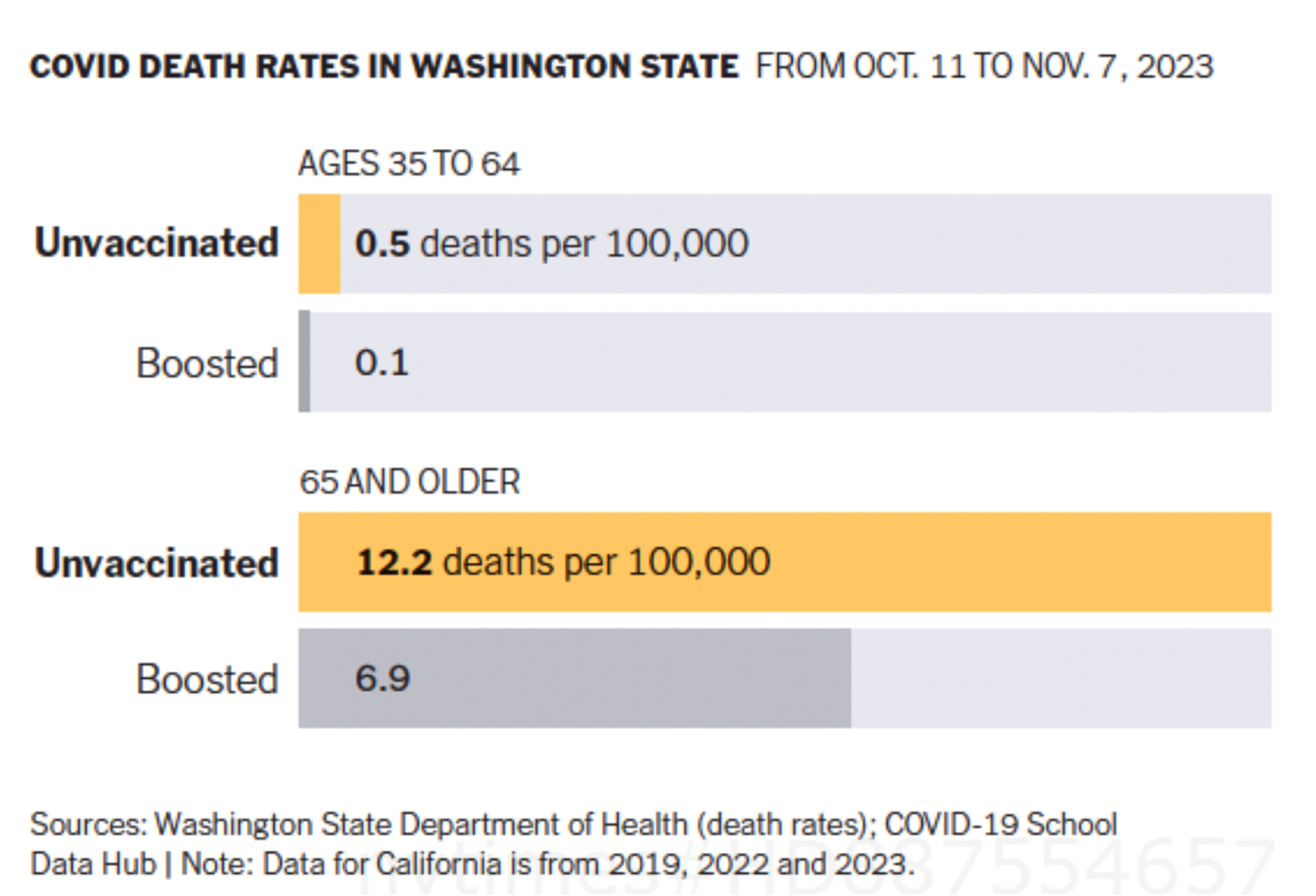
Multiple state level data, such as Washington’s below, indicate the protection from death with a booster, almost halving the rate in people age 65 and older
Evolution of the Virus
The JN.1 variant took over globally and a number of subvariants (JN.1.11.1, JN.1.18, JN.1.13, JN.1.18) are showing up with added spike mutations such as R346T and F456L, but without signs of wastewater levels on the rise or other concerning metrics.
But BA.2.87.1, as mapped below, is the major “Omicron-like” event out there that has been the subject of 5 recent papers/preprints (here, here, here, here and here). That, in itself, should tell you it’s a variant of interest. It’s chock full of new mutations compared with the variants that came along previously, and many of these are deletions (blue below)..

In itself, it is not a threat as there’s no sign it is more immunoevasive or transmissible. In fact, the consensus it that it’s less evasive of our immune response, the current booster works to achieve good levels of neutralizing antibodies, and some of the monoclonal antibodies that were previously found to be resistant to earlier variants may be effective again. That’s great news. But as Yunlong Cao and his team appropriately warned us, “BA.2.87.1 may not become widespread until it acquires multiple [receptor binding domain] RBD mutations to achieve sufficient immune evasion comparable to that of JN.1.”
It’s much too early to know whether (and when) this will take place, but after 4 years if there’s anything to predict, it is that the virus will find its way (through selection) to infect more hosts and repeat human hosts.
Protection from Vaccines
A big study was reported yesterday that addressed the question of protection from Covid shots against blood clots—deep vein thrombosis and pulmonary embolism, heart attacks, strokes, and heart failure. The data are from 3 countries—UK, Spain and Estonia, from electronic health records of over 20 million people. All these outcomes were reduced by prior Covid vaccination compared with no vaccination, especially in the first 30 days after an infection, but many showed durable protection out to 1 year follow-up (stroke, TIA, heart failure, DVT, PE).
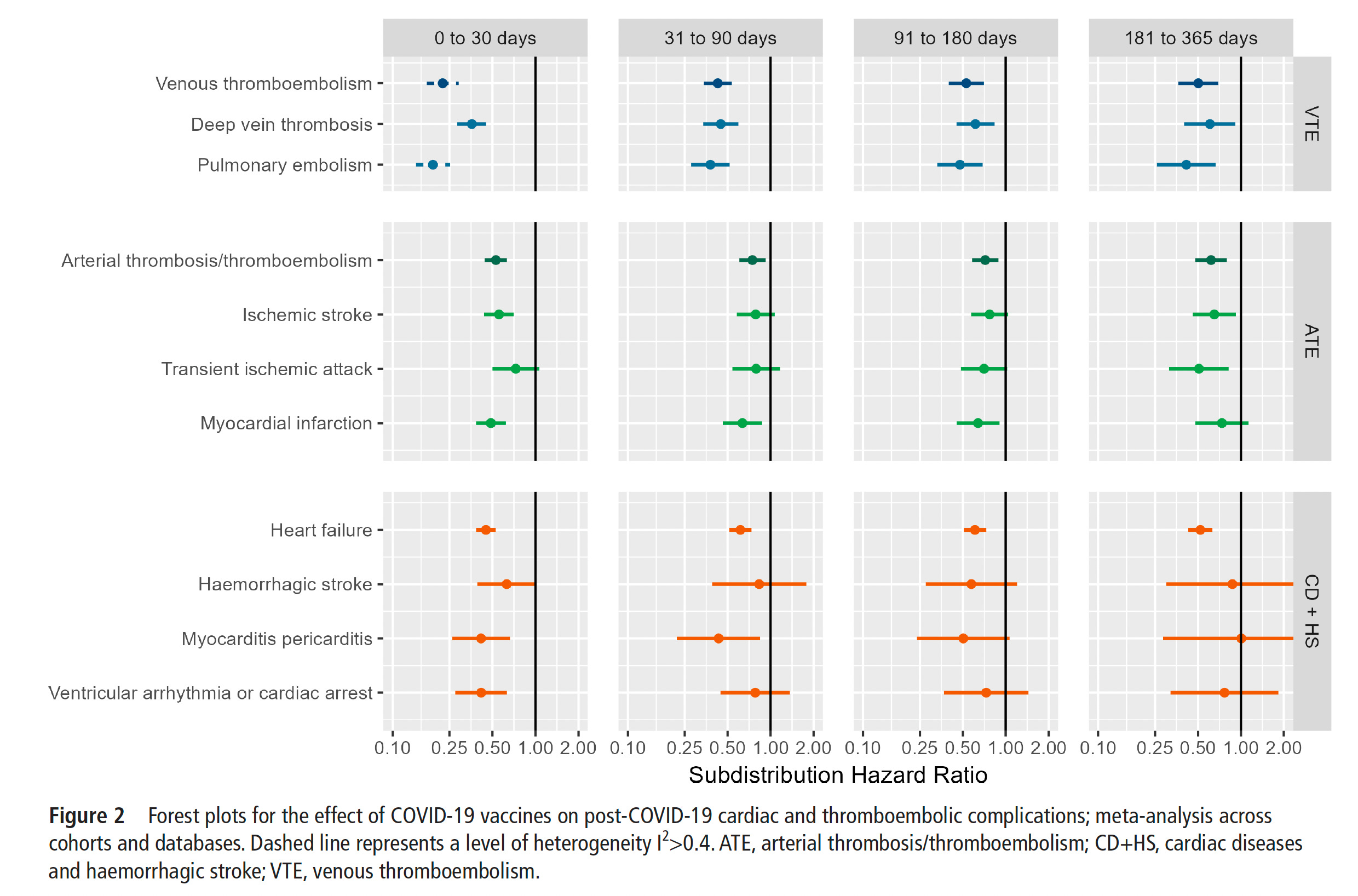
This is different from the 40-50% protection of vaccinations vs Long Covid symptoms. It’s specifically addressing major cardiovascular outcome protection from being vaccinated. Major welcome news!
One More Thing
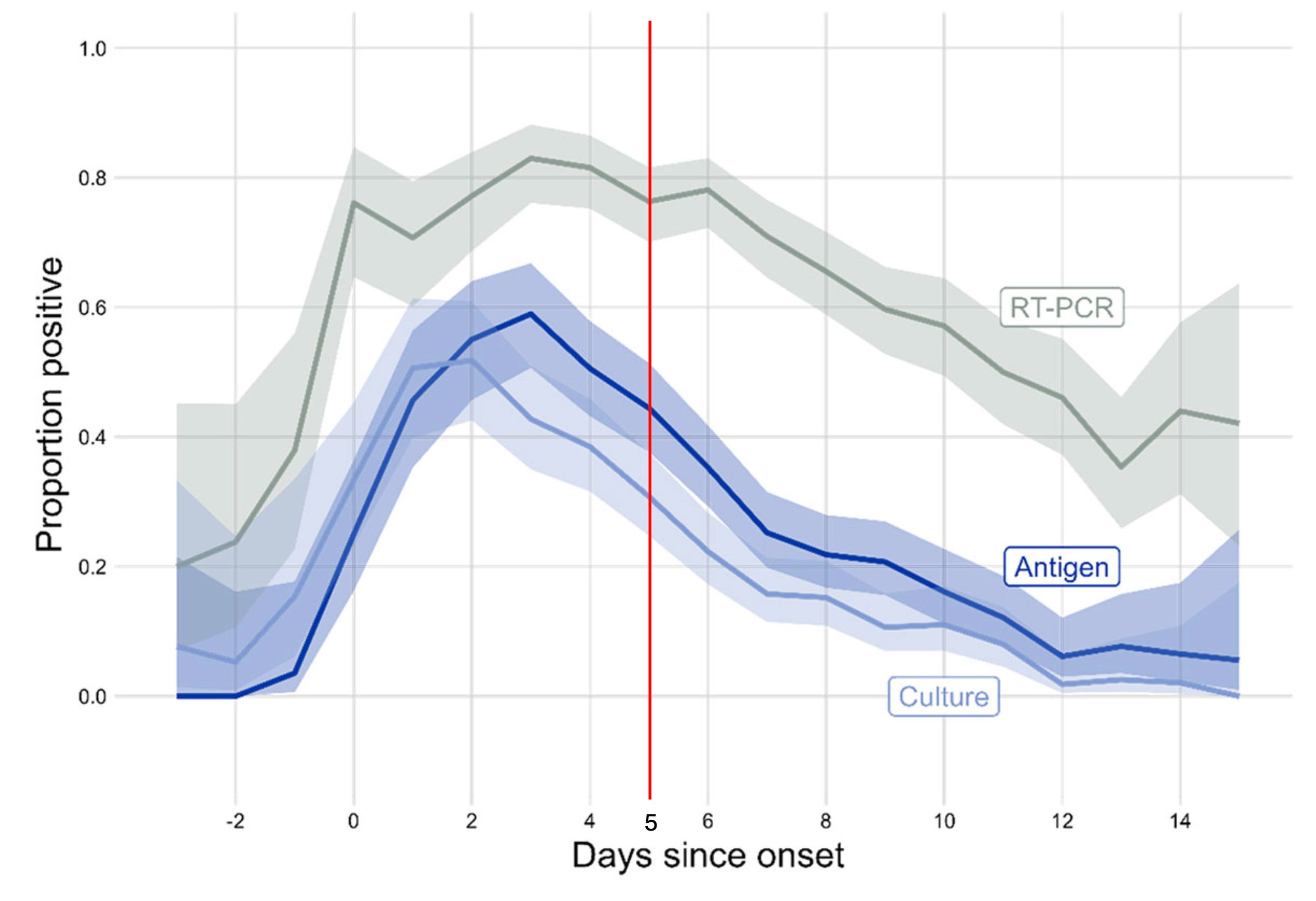
I remain very disappointed and surprised by the recent change (1 March) of CDC policy towards isolation, without regard to using rapid antigen tests. Their own data shows that at least 1 in 3 people will still be infectious at 5 days after symptom onset! That’s by culturable virus, the gold standard, which tracks very closely with the rapid tests. To reduce infecting others, especially high risk vulnerable individuals, no less adding to the toll of Long Covid, rapid tests should be used before people circulate.
Thanks for reading Ground Truths and please share the post to your network of friends and colleagues if you found it useful.
Eric, thanks as always for your comprehensive summary. I guess I shouldn’t be surprised that few people, even those who’ve kept up with vaccinations, seem to be aware of the CDC’s current recommendation for a repeat booster for individuals who are 65 or older.
I don’t know how many people use the CDC’s website, but I find it confusing, with too many links. Key information should be presented more prominently. They should consider a section that lets you enter items that apply to you (age, prior vaccination or infection, and so on) and then provides a recommendation.
Thank you for the updates, Eric. I try to pay attention to the latest recommendations and research re: COVID-19. I have been very careful, getting all of the recommended vaccines and utilizing rapid testing a few times when I had respiratory symptoms. (All tests were negative.) I have not had the infection and am very grateful as I know that it increases the chances of developing
Long Covid. I too was disappointed by the CDC’s recent change in guidelines re: number of days of isolation before returning to work or school. As a former teacher, I felt that the guidelines could definitely increase risk of transmission of the virus in schools.