
Covid Brain
Two important studies this week shed new light on after-effects, 1-year out, and other key updates
Since Ground Truths got off the ground (no pun intended), I’ve written much about the impact of Covid on the brain (such as here and here) and discussed on my podcast with Michelle Monje, a leading researcher on neuroinflammation and this condition and with Akiko Iwasaki, one of the world’s leading immunologists. But this week, 2 new publications have substantially added to our understanding of the extent that Covid can impair cognitive function across the full gamut— from young, healthy individuals with mild infections to older, hospitalized patients with severe Covid. In this post, I’ll review the 2 new reports and some related advances in the field.

Hospitalized Patients With Severe Covid
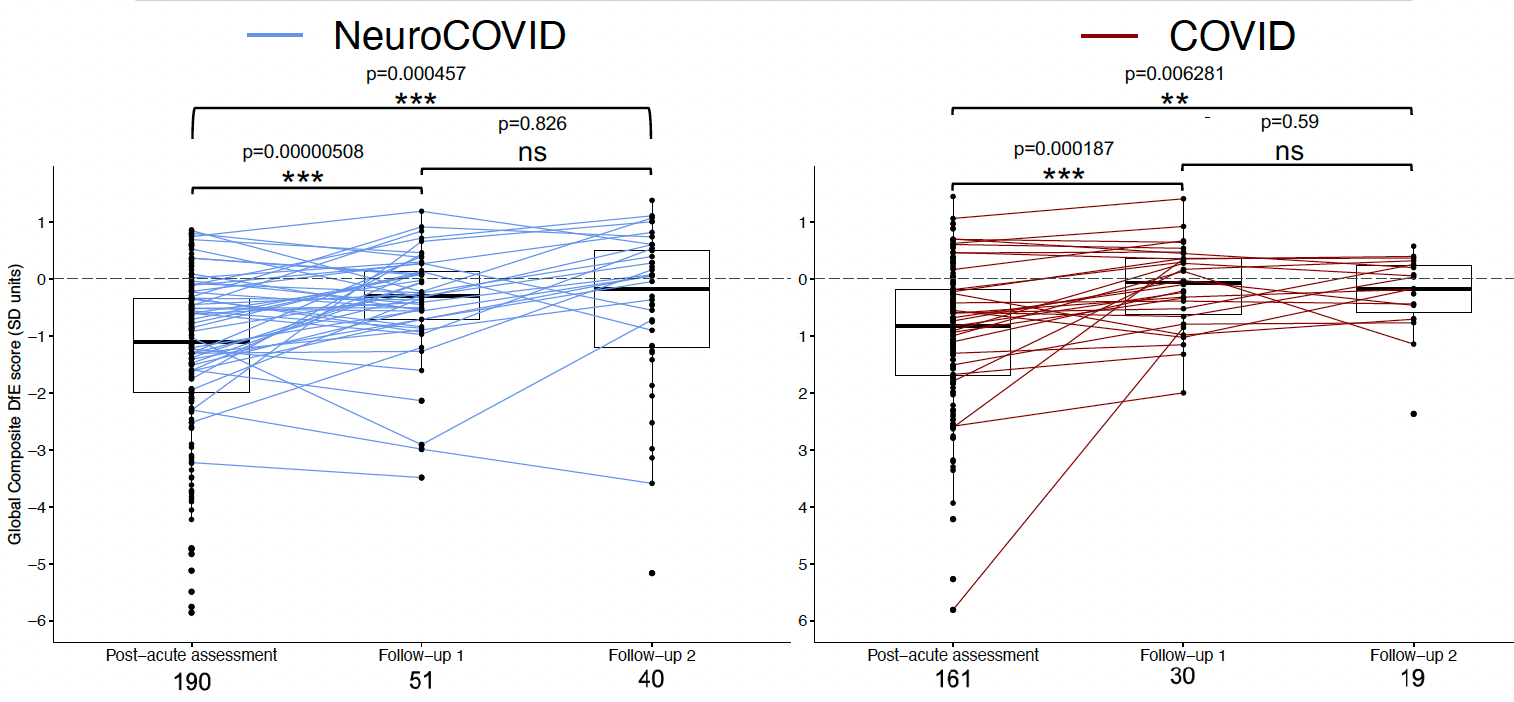
Greta Wood and her colleagues at University of Liverpool published a seminal paper in Nature Medicine— a prospective, multi-center, systemic assessment of the brain by MRI imaging, blood brain biomarkers of injury, and cognitive performance—in 351 individuals with Covid and nearly 3,000 matched controls. The cases had no prior neurologic disease, were an average of 54 years of age, and only 19% had been vaccinated. More than half (54%) had a neurologic or psychiatric complication during their Covid hospitalization, considered the NeuroCOVID subgroup; the remainder were defined as the COVID group. Controls were age, sex and educational level matched.
Here is the graph of cognitive scores and recovery trajectory for the post-acute assessment, Follow up-1 (median 111 days) and Follow-up 2 (median 384 days). Both groups showed some signs of recovery. Note the number of individuals at Follow up 2 were limited.
The main findings, some of which are summarized in the graphic below, were:
Significant reduction in cognitive performance scores in all of the 8 case clusters compared with controls, especially executive function, worse among those by severity of Covid, abnormal mental health status of encephalopathy during the acute phase.
Substantial and persistent, ongoing increase in brain injury markers in the COVID and NeuroCOVID patients—NFL, Tau, GFAP and UCH-L1. Serum GFAP is expressed by astrocytes, which are key immune mediators, and supports the mechanism of injury is immune-mediated.
Gray matter atrophy, particularly seen in the volume of the anterior cingulate cortex.
Subjective symptoms of cognitive impairment were correlated with objective findings. In addition, depression was frequently reported.
By the Global Deviation from Expected (GDfE) score assessment, the cognitive deficits were equivalent to a 20-year acceleration (e.g. performance of a 50-year old at the 70-year old level)
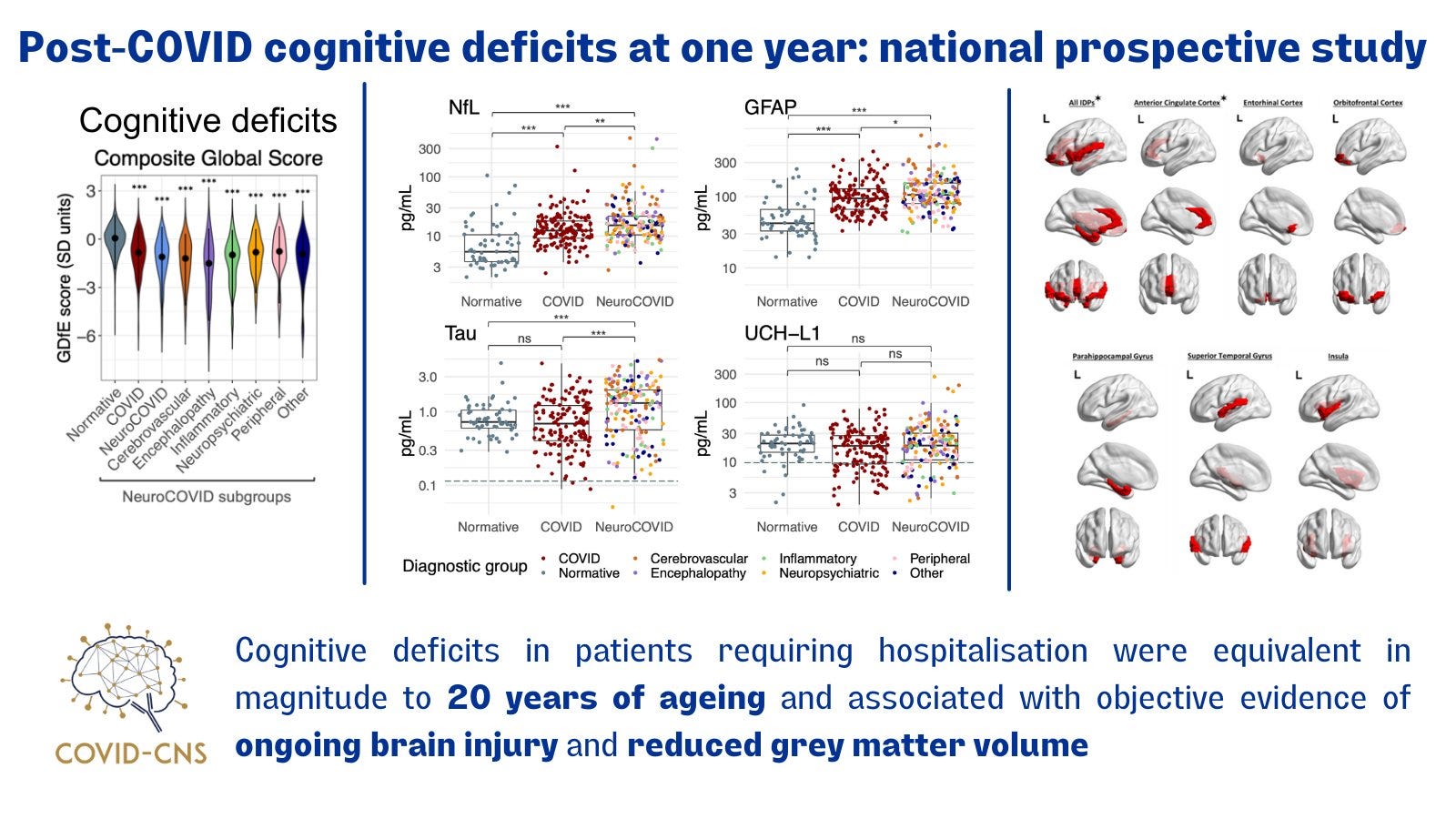
Cognitive deficits were more likely in patients with a neurologic or psychiatric complication, older age, more comorbidities, There was some protection noted with higher educational level and in-hospital treatment with dexamethasone.
The Healthy Volunteer Study
William Trender and colleagues at Imperial College London published the results of a prospective challenge (wild-type SARS-CoV-2 inoculation) study of 34 young healthy (aged 18-30 years), seronegative (uninfected), individuals ; 18 showed signs of infection and 16 did not. The goal, which had not been previously undertaken, was assessment of cognitive function and memory at multiple time points after the virus challenge, at 30. 90, 180. 270 and 360 days. Of the 18 cases with infection, only 1 was asymptomatic; all the others had mild Covid. You can see the significant difference in cognitive scores between infected and uninfected below, out to 1 year. The top is a heat map representation of the data and the bottom panel plots the median and standard deviation scores.
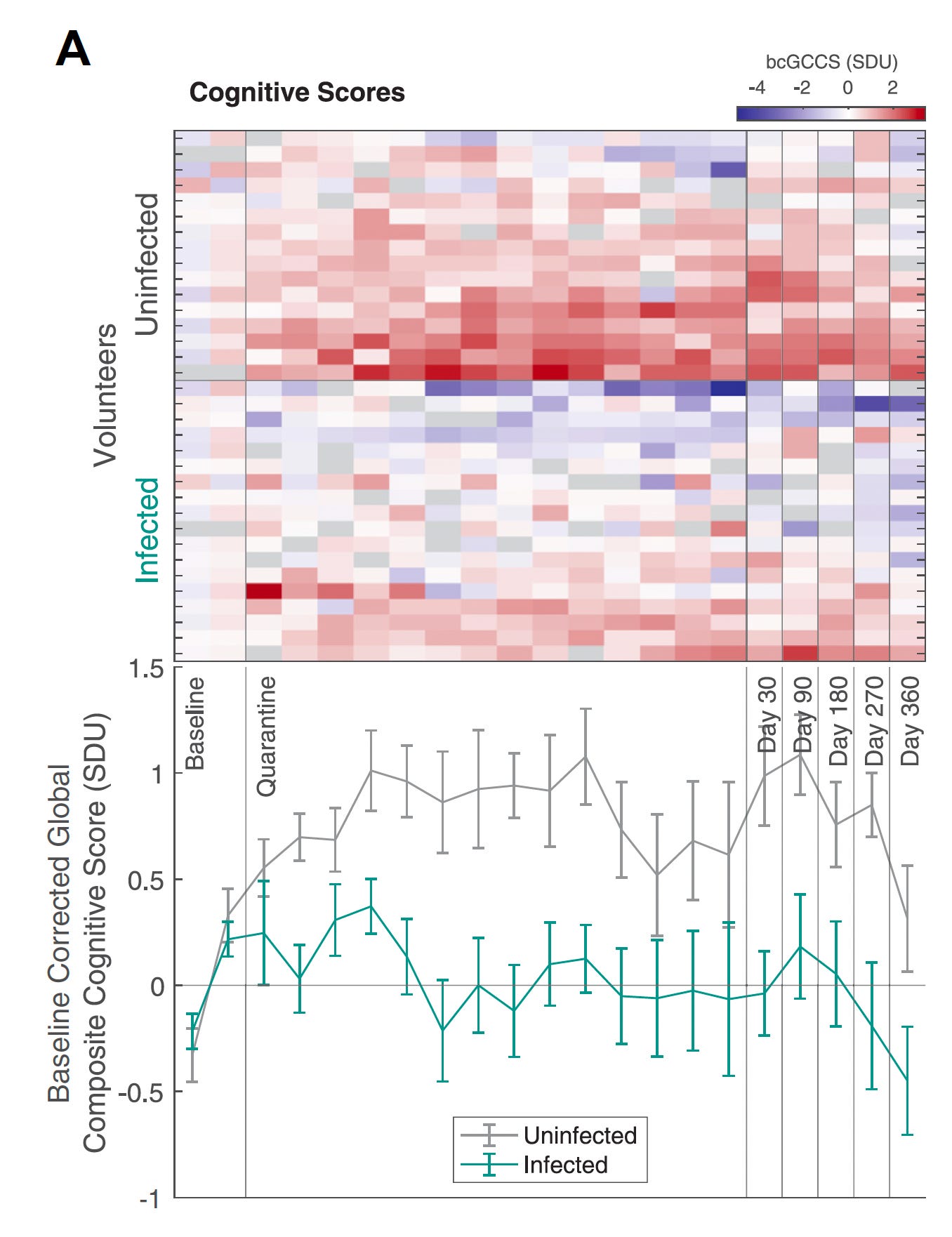
Unlike the study in hospitalized patients, there was a dissociation of subjective versus objective assessment, with none of those infected perceiving deficits in executive function or memory. The longer the viral load persisted, the worse the cognitive score. This is a small study, since infection challenge studies are extremely difficult to perform, and raise ethical concerns. Please note the protocol was rigorously reviewed by the UK Health Research Authority’s Ad Hoc Specialist Ethics Committee. Potential, uncharacterized baseline differences in the individuals infected vs uninfected could be confounders for interpretation of the results.
Related Progress
Risk of Reinfections
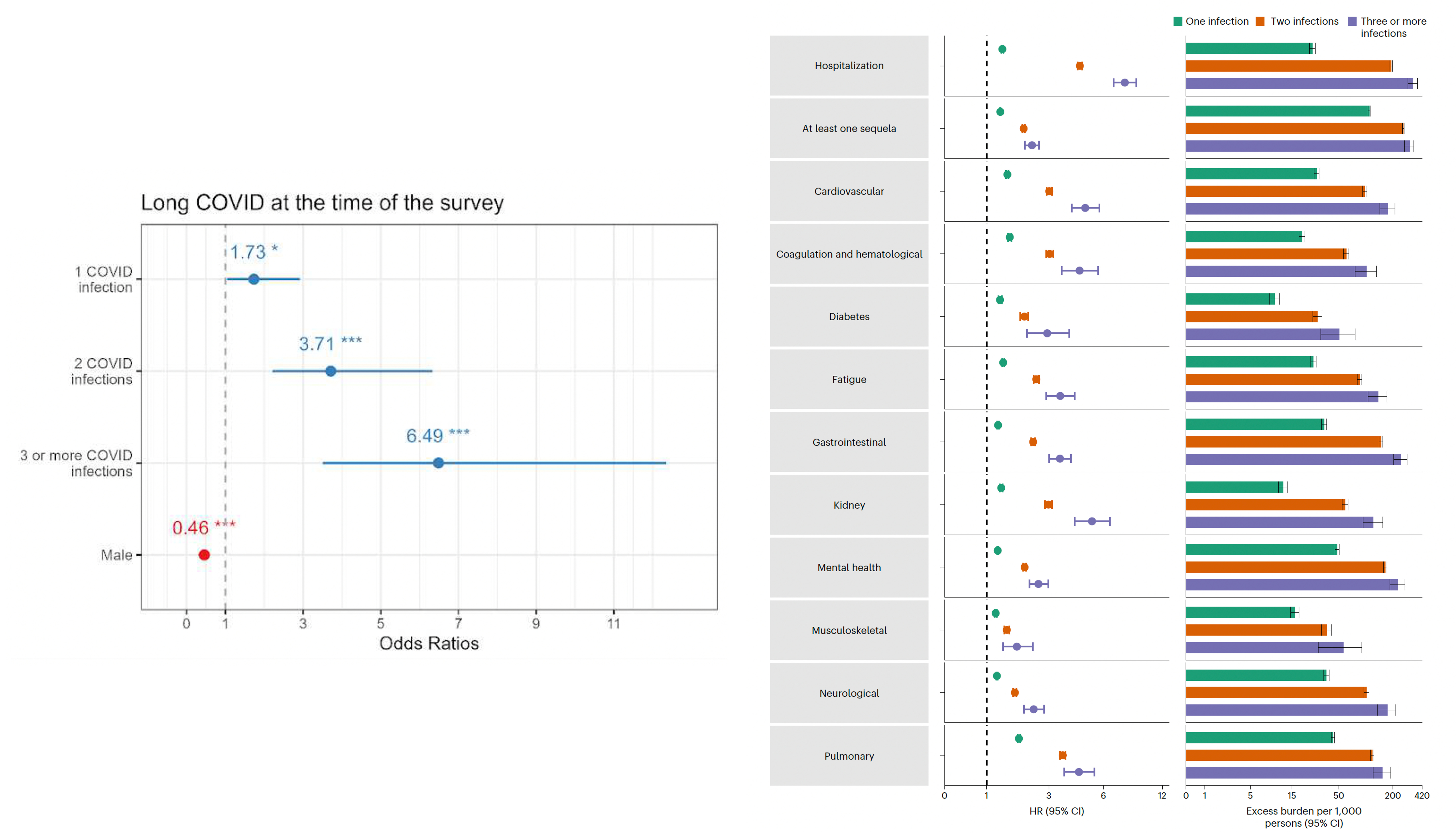
The Patient Led Collaborative Group, in an impressive preprint, found, among over 3,300 participants completing online surveys, that, once again there was a “dose-response” of Covid infections with the risk of developing Long Covid (left panel below), corrected with worse symptoms and impair physical function. While the participants were predominantly women and younger, there is striking concordance with older males in the Veterans Administration huge data resource.
Previously, from the VA dataset, Ziyad Al-Aly and colleagues showed a very similar increased risk—both in magnitude and direction— for 2 and 3 Covid infections and the development of Long Covid by organ system, as seen in the right panel below.
Results of a Nasal Vaccine
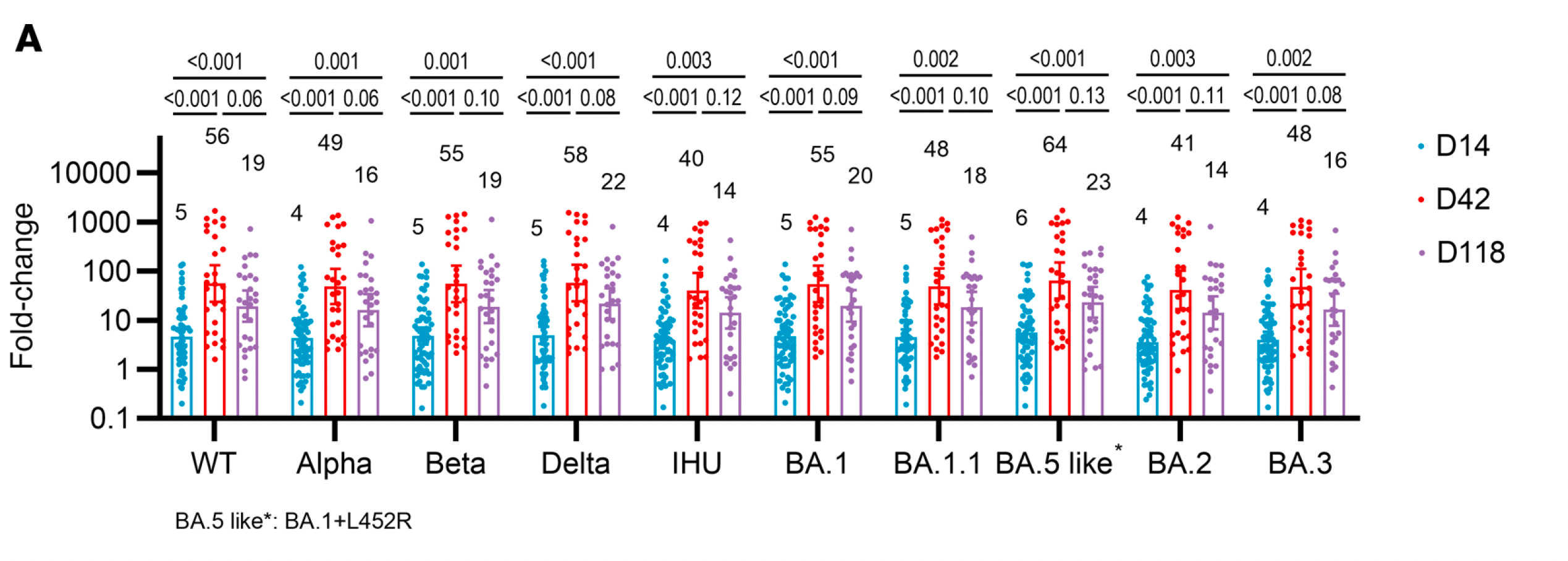
In JCI Insight, in China, 128 health care workers were given 2 doses of a nasal vaccine spray, one month apart, at the end of 2022, after prior vaccination. The vaccine is an adenovirus vector that is replication-incompetent, directed against the Omicron BA.1 spike. As it turns out, this nasal vaccine induced more than 50-fold increase in spike-specific IgA secretly antibodies, indicative of achieving potent mucosal immunity. This was seen and consistent against 10 different variants of SARSCoV2! (Graph below). Moreover, while the first dose didn’t offer high protection from infection (43 of 75 participants got infected) or transmission, after the second nasal dose 86% maintained uninfected status 3 months out (at a time with high levels of circulating virus in a high-risk group of healthcare professionals). There was screening for asymptomatic infection using nucleocapsid antibodies, so 2 of the individuals exhibited that add in the mix of very high level of protection from infection afforded by the 2 doses, at least in this small sample. But it ‘s the first clinical data of a nasal vaccine to show protection from infection. That’s a welcome finding to help mitigate the prevailing big hole left from shots for protection from (re)infections and spread.
Type 1 Interferon Auto-Antibodies
About 10% of people who develop severe Covid have pre-existing autoantibodies to Type 1 interferon (our first line of immune defense), which doesn't get diagnosed. Now there's a simple assay, a new report in PNAS, by Jean-Laurent Casanova and colleagues at Rockefeller University, who previously described the frequency and susceptibility of people with these self-directed antibodies. It's also relevant for other life-threatening viral illnesses, and these Abs exist in ~100 million people worldwide. Furthermore, we keep categorizing people as “immunocompetent” or “immunocompromised” but that’s wrong! Many people have specific immunologic liabilities that are not assessed or have not yet been discovered.
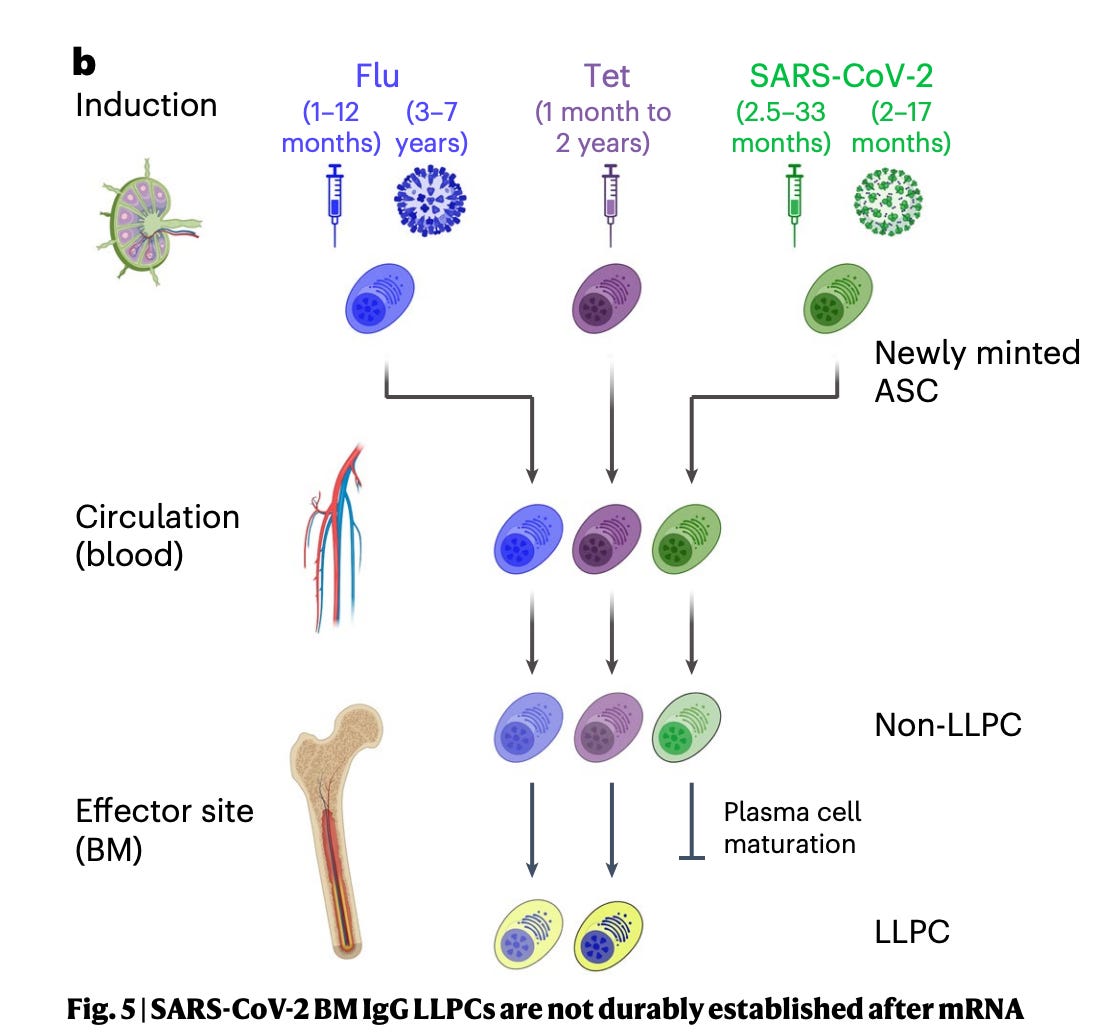
mRNA Vaccines and Long-Lived Plasma Cells
A paper in Nature from Emory University researchers is the first to find the lack of mRNA vaccine induced long-lived plasma cells (LLPC) vs SARS-CoV-2 as compared with the durability of mRNA shots vs flu or tetanus. We don’t know whether this is the case with other vaccine formulations, and this finding was not affected by hybrid immunity (an mRNA shot plus infection). Until we know more, it may well be related to the challenge of SARS-CoV-2 spike’s protein. See Akiko Iwasaki’s excellent thread for more details.
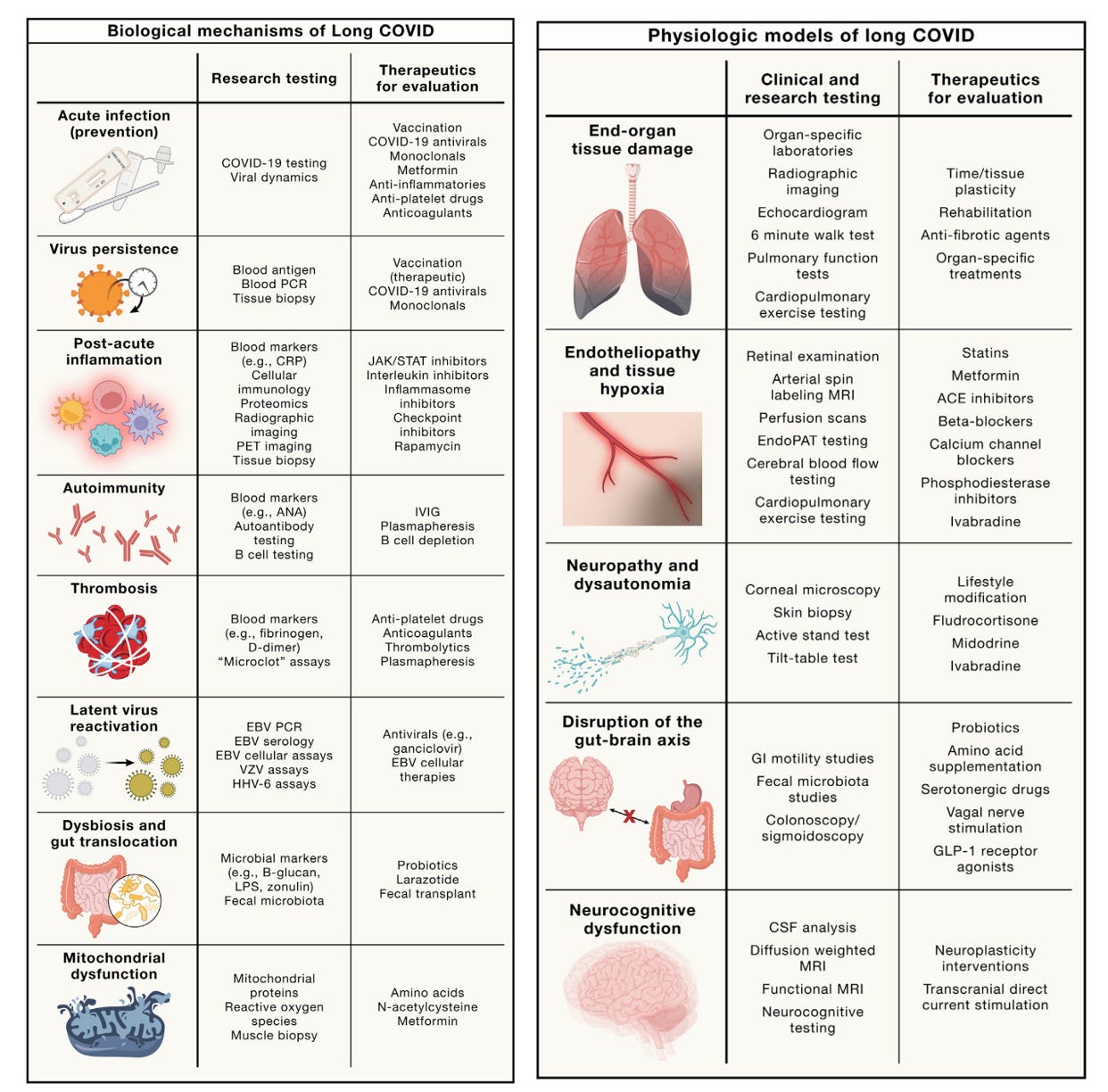
A new Long Covid Review
A systematic review by Michael Peluso and Stephen Deeks in Cell maps out the mechanistic underpinnings of Long Covid and how to target each one. it’s masterfully done and open-access.
If you have a chance, please review Professor Christina Pagel’s latest substack post, on the UK current wave and the link to the remarkable video testimony by Dr. Kevin Fong, at the UK Covid Inquiry.
Summing Up
The potential of a Covid hit to the brain, affecting cognitive function, has been clearly reinforced by the 2 new studies, with the whole spectrum of mild cases among healthy, young, people to older, severe Covid hospitalized patients. Both these studies have many limitations, but the backdrop of now well over 20 preceding publications on the brain and Covid can be regarded as the priors that make this real. For the challenge paper described above, it may represent be the best case scenario, since there was continued exposure to circulating virus after the initial infection. On the other hand, the participants in both studies were largely unvaccinated (zero in the challenge study and 19% in the hospitalized study), so we may be looking at a pre-vaccine era landscape and one of early variants rather than the ones circulating these days.
Brain Covid, manifest by some objective reduction of cognitive performance, even after mild cases in young, healthy people, yet not perceived by the person infected, is worrisome enough, no less what has been consistently described with severe Covid, dating well back to the 2022 UK Biobank study with paired MRI imaging (in cases and uninfected controls) and structural evidence of brain atrophy, a foundation for the new study reviewed above (and cognitive deficits). We still do not have a good handle whether this is eventual reversibility of the hits (cognitive and structural) of if they are persistent. The severe Covid data suggesting brain injury biomarkers were persistently abnormal at 1 year is not at all reassuring.
This pattern is so different from other respiratory viruses that we are accustomed to being to, such as influenza, and suggests that the tropism of the virus to the central nervous system and resultant pro-inflammatory effects are not uncommon features of Covid. But you wouldn’t know that by the cavalier lack of regard for use of mitigating measures among most people today. Beyond that, our blatant lack of priority for getting a nasal vaccine here in the United States that seems to block infections well and works across all variants. We should have had one or more of these commercially available 2 years ago, but there is no sense of urgency or willingness to step up with resource commitment. Sadly, we’re into deep denialism and the delusion that we’re beyond the threat of Covid.
I believe the new findings here, once again, behoove us to take the threat of SARS-CoV-2 much more seriously, just now coming down from a major wave related to the KP.3 and KP.3.1.1. variants, and undoubtedly another one to come in the months ahead, perhaps driven by the XEC variant (see Ryan Hisner’s thread on that one) that is, for unclear reasons, picking up steam in some places around the world, including the United States.
If you haven’t, please consider getting the new booster. Extrapolating from the published data for the previous XBB.1.5 booster in 2023 (that I’ve reviewed in prior posts) , it should provide some (~50%) protection from infection for 4-6 weeks, protect well (>80%) against severe Covid for 4-6 months, and will help reduce the risk of developing Long Covid. We need to use our brains, rather than to leave them vulnerable to this god-awful virus.
*********************************************
Thanks for reading and subscribing to Ground Truths.
If you found this interesting please share it!
That makes the work involved in putting these together especially worthwhile.
All content on Ground Truths—its newsletters, analyses, and podcasts, are free, open-access.
Paid subscriptions are voluntary and all proceeds from them go to support Scripps Research. They do allow for posting comments and questions, which I do my best to respond to. Many thanks to those who have contributed—they have greatly helped fund our summer internship programs for the past two years.
Thank you so much for your vigilance on the dangers of contracting COVID, which all too many would prefer to forget. Thanks also for your persistent beating of the drum on getting a nasal vaccine. It is shameful that we have failed so far in the US to provide sufficient resources to get this done.
Your work and writing on the dangers of COVID are invaluable. But it would be so appreciated if you could also write about possible therapies for those suffering from long COVID- especially the fatigue and cognitive challenges. Hope for recovery is much needed for this group.