


Pandemic update, 31 October 2022
The 1st of daily/frequent brief updates
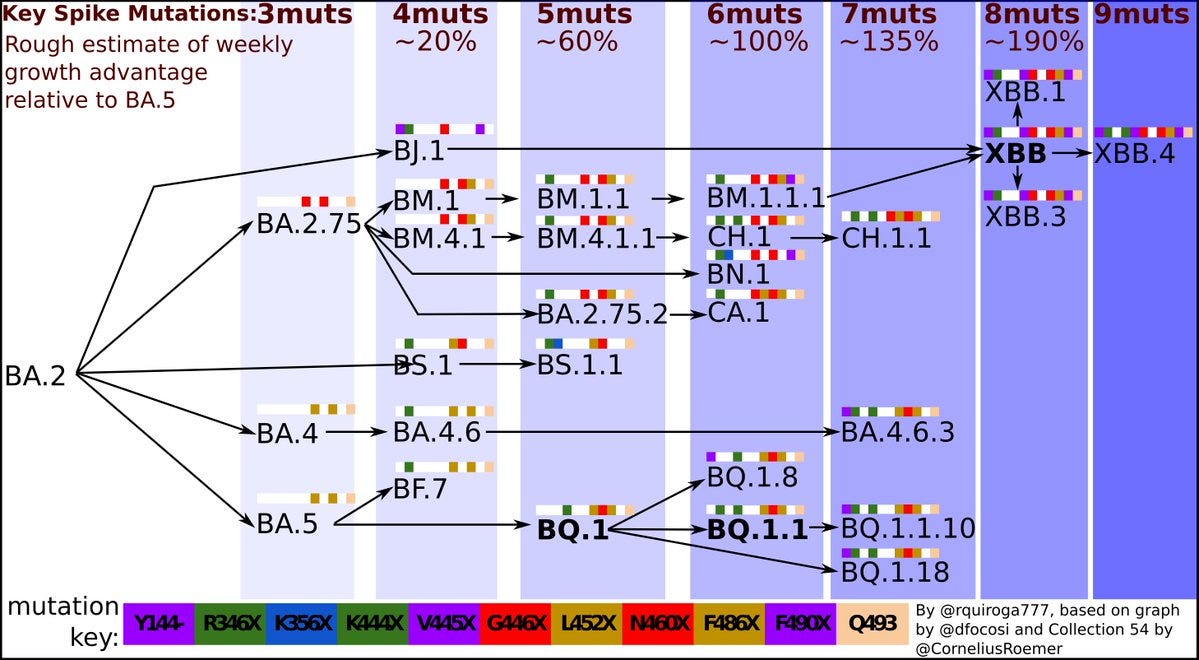
To summarize the key points today, there was an important new preprint by Yunlong Cao’s group showing that the new variants with marked immune evasive properties are rapidiy picking up additional mutations. We’ve been worried about BQ.1.1 but now there’s BQ.1.1.10 which shows more evasion (than BQ.1.1) after 3 CoronaVac shots plus a BA.5 breakthrough infection (below). There’s also XBB.1, XBB.3 add ons (beyond XBB), along with BA.4.6.3, CH.1.1, that similarly take immune evasion to a higher level than what we’ve previously seen.

The growth advantage compared with BA.5 is substantial, such that for each of the convergent mutations that the swarm of variants are accruing, the growth advantage increases, as nicely shown in this graph by Rodrigo Quiroga. In the early watch of these converging mutations seen in the new variants it was 4 or 5, but now we’re getting up to even 8 or 9 mutations with almost doubling of the growth advantage vs BA.5.
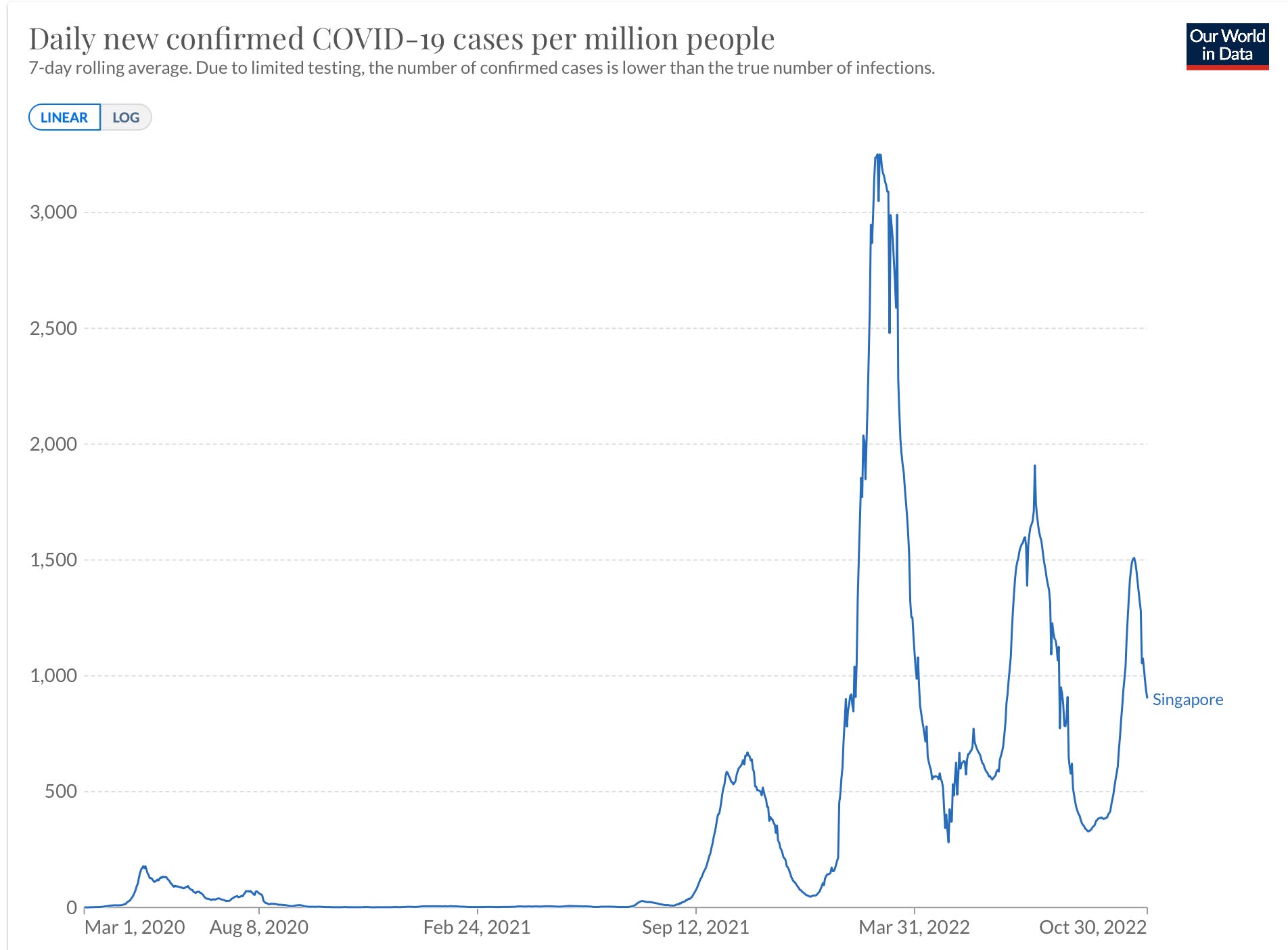
Has this induced clinical impact yet? The only place that has seen a wave due to one of these new variants is Singapore (graph below), which is now in descent, and did not have a major corresponding spike in hospitalizations or deaths. XBB is dominant in other countries like Bangladesh and India, which have not shown any spike in cases or deaths to date. Keep in mind that the vaccination and booster rate in Singapore is extremely high (boosters were the original, not bivalent), whereas the prior Covid infection rate in the other countries that have had high XBB exposure is also high.
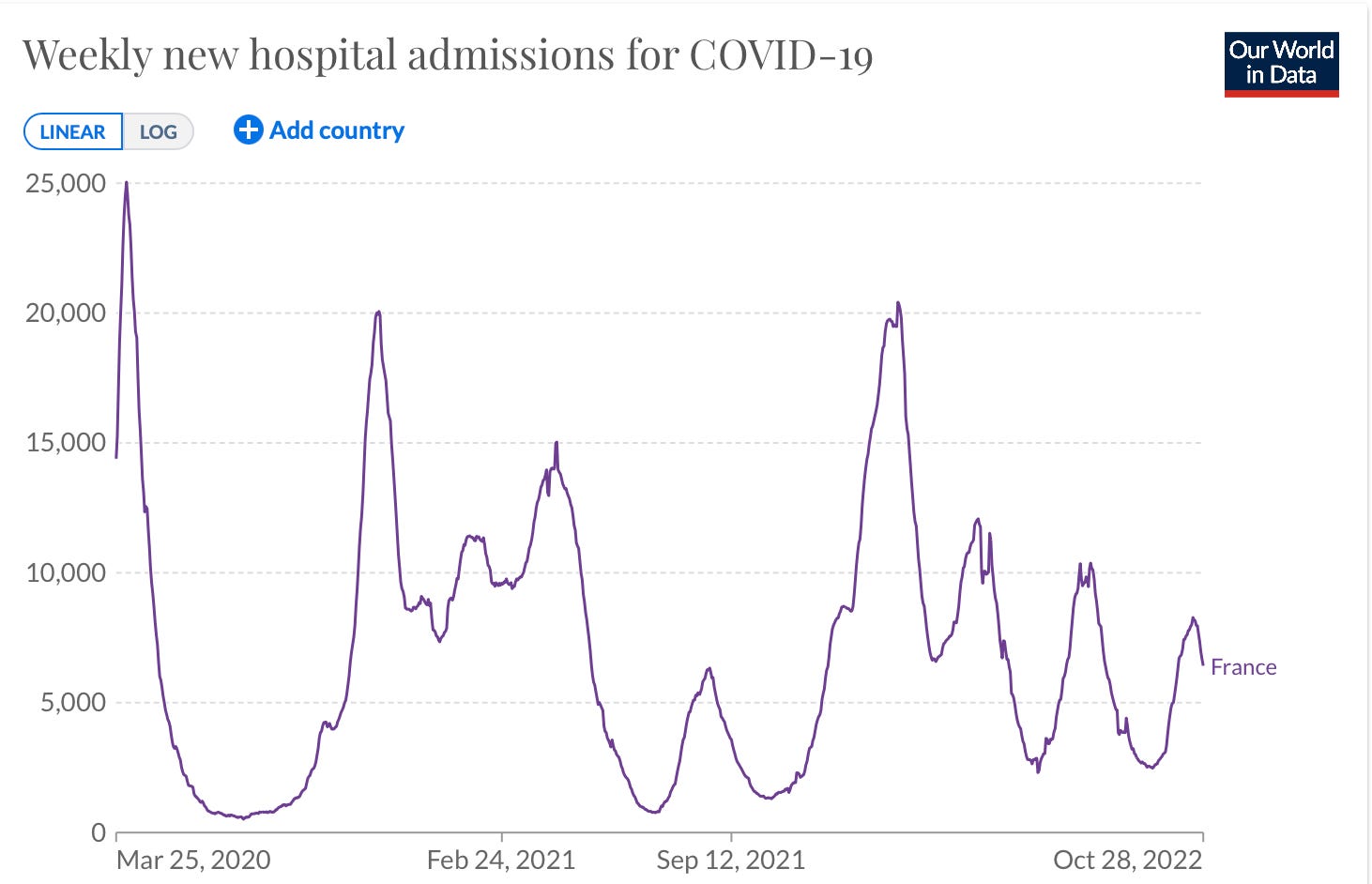
We haven’t yet seen countries with BQ.1.1 reach dominance. France is the closest but has yet to exhibit an increase in cases or hospitalizations (in contrast, see below), which is also reassuring. But we will need to see how this particular variant fully plays out in many countries before saying that the immune evasion properties are not correlating with a surge of infections and adverse outcomes.
In the United States, BQ.1.1 is 13% as of the last CDC update
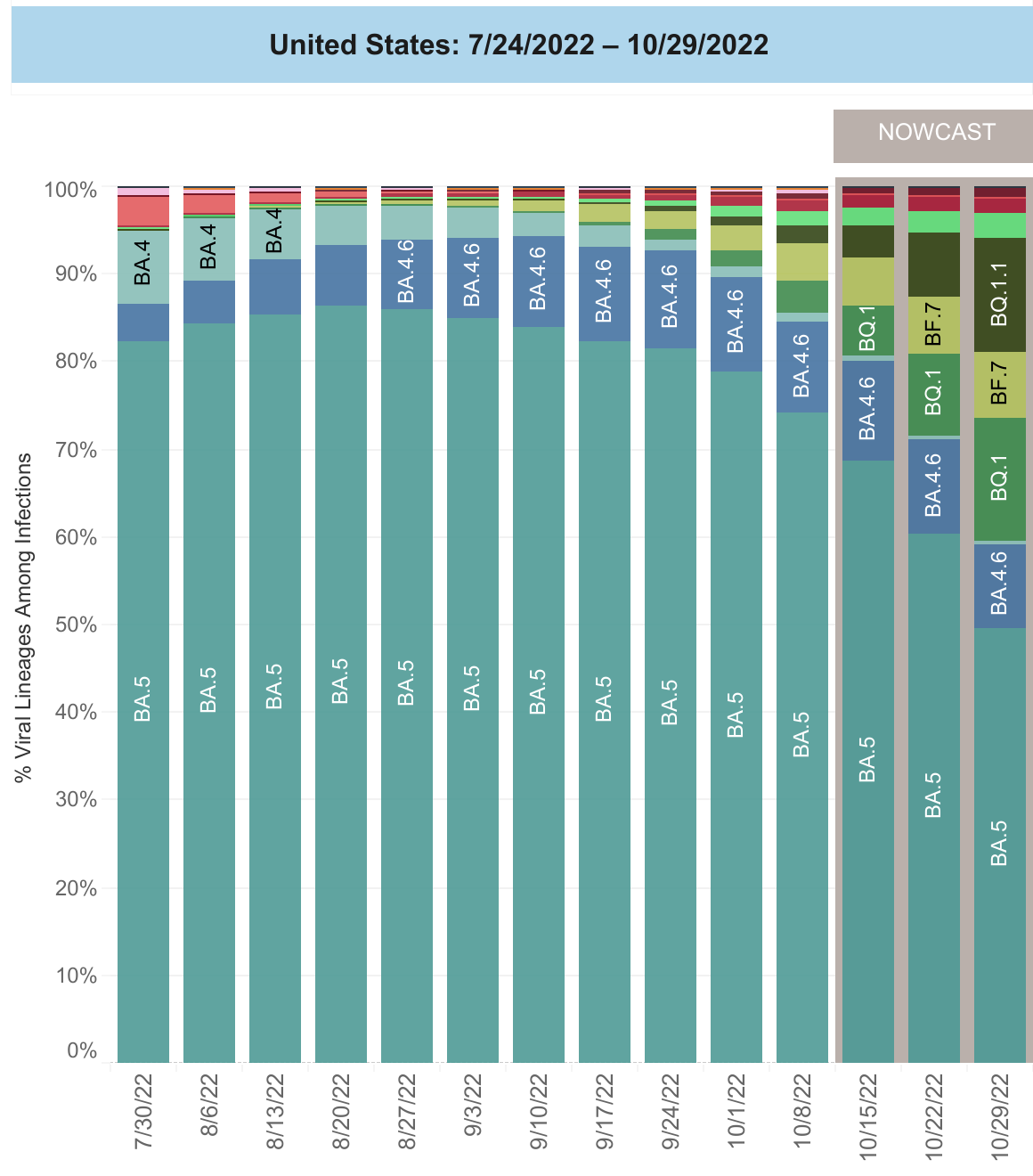
so we have weeks to go before it accounts for >50% of new cases. It isn’t yet clear how well cross-reactivity with BA.5 or prior Omicron lineages (BA.1, BA.2, BA.2.12.1, BA.4.6) will help provide protection vs BQ.1.1x and our booster rate, especially in people of advanced age, is considerably lower than most countries in Europe and Asia.
Another point of mention today is we learned that Dr. Rochelle Walensky, CDC Director, had rebound after a recent Covid infection treated by Paxlovid. Although Drs. Fauci and Walensky, and the President, have had rebound, and it is not rare by any means, we will be publishing data from a prospective, systematic study soon that rebound is not frequent and is not any reason to withhold the therapy in suitable candidates. Wishing Dr. Walensky a rapid and complete recovery.
In the weeks ahead, it is smart to anticipate a new wave of spread. If you haven’t had a recent booster (within 6 months), it would be wise to get one. Not to worry that the bivalent booster may not be any better than the original one—it will still augment and broaden your immunity and protection against severe disease. And the benefit is very important if you’re age 50 and older, with >90% reduction death and >80% reduction hospitalization. Furthermore, since we can’t rely on vaccines/boosters to significantly prevent infections, use of N95/KN95 masks in the right settings is important for maintaining protection.
With twitter’s instability, I’ll try to post a quick summary like this on a frequent if not daily basis.
Thanks for reading.