
In just a week’s time, we’ve learned more than we’ve had in many months of the Covid pandemic. There’s been a flurry of new reports covering critical holes in our knowledge base. I’m going to briefly review here the new reports on (1) prevalence; (2) mechanisms and biomarkers; and (3) potential treatments.
Prevalence
While there have no shortage of studies that describe symptoms of Long Covid and estimate its frequency, with wide ranges from 5-35%, we finally have one that captured symptoms in thousands of people before they were infected and followed them for months, with age and sex-matched controls who remained uninfected. 12.7% or 1 in 8 people who had Covid were considered to develop the condition, since there were 21.4% with persistent symptoms (3-5 months) in the Covid group compared with 8.7% in the control group. The excess in core symptoms documented included chest pain, difficulties with breathing, painful muscles, general tiredness, and headaches.
The cohort from the Netherlands population wasn't diverse, the study was pre-Omicron, most people were unvaccinated, and it did not include assessment of neurologic symptoms such as brain fog, or those related to mental health. There have been reports that Long Covid is less prevalent with Omicron and reduced by vaccination, but none have prospectively captured symptom data before infection. Whatever the current prevalence of Long Covid is with BA.5 in people who have been previously fully vaccinated remains uncertain. It’s very likely lower, but even high single digits represents an overwhelming burden of chronic morbidity and, in all too many people, disability. I recently discussed this study and the current status of Long Covid with Michael Holmes on CNN.
On the good news front, while that Netherland study was in adults, a recent report in children with controls suggested that Long Covid in kids is of low prevalence. While it had matched controls, there was no baseline ascertainment of symptoms and prospective follow-up. We’ll need more studies in children and adolescents to get at its true prevalence, but it’s low, and there’s a gradient of even less with young age that has been consistently reported. Of note, even though Long Covid in kids appears to be rare, a new CDC report suggests there is a doubling of serious sequelae among the children affected, including a doubling of pulmonary embolism, myocarditis or cardiomyopathy, venous thrombosis, along with an increased risk of diabetes and kidney damage.
Mechanisms and Biomarkers
One of the best studies of Long Covid was just released in preprint form from a 2-year combined effort at Yale School of Medicine, led by my friend Prof Akiko Iwasaki, and Mount Sinai School of Medicine, led by David Putrino. While the cohort assessed was not large (215 individuals) the data assessment was remarkably deep and multi-dimensional, with controls who were healthy (HC), convalesced without Long covid (CC), and Yale health care workers (HCW) without Long Covid. (LC).
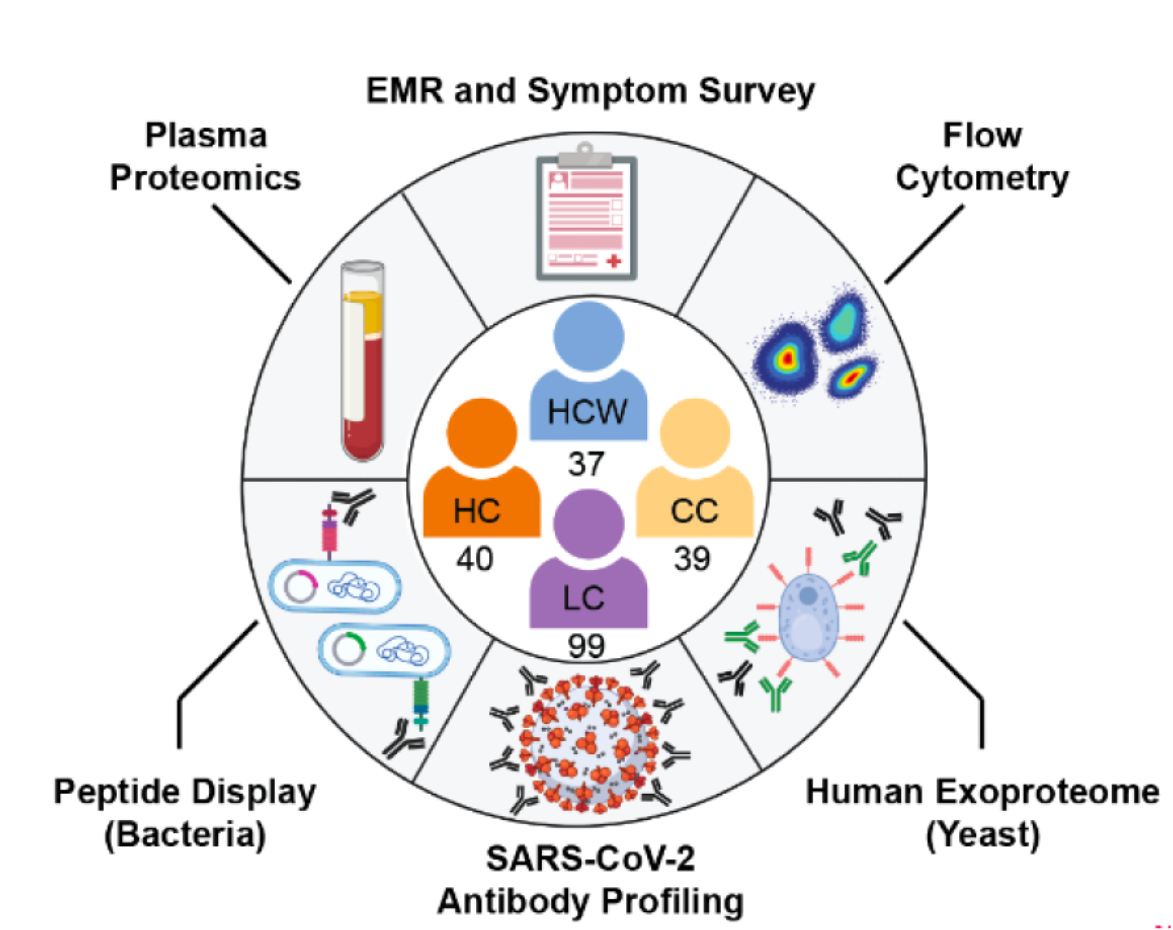
The layers of data included:
✓ Flow cytometry of blood mononuclear cells
✓ Memory T cells, CD4+ and CD8+ T cells
✓ Antibodies to the SARS-CoV-2 spike protein (with bindings sites, aka epitopes, defined)
✓ Auto-antibodies to proteins (extracellular, exoproteome)
✓ Antibodies to Epstein-Barr virus (EBV) and Varicella Zoster virus (VZV)
✓ Various hormones including Cortisol and ACTH
The notable findings include (1) 3 symptom complex clusters and patient reported outcomes identified Long Covid with 94% accuracy; (2) Herpes (EBV, VZV) virus reactivation; (3) multiple antibody + cellular immune markers consistent with heightened immune system activation. These all replicate and extend prior findings.
Notable in this report was the use of machine learning A.I. to let the data talk, tell us whether there was a driving feature from the extensive data collected that might separate Long Covid individuals from controls. And it turned out there was a driver and it was cortisol, with the relevant data summarized below.
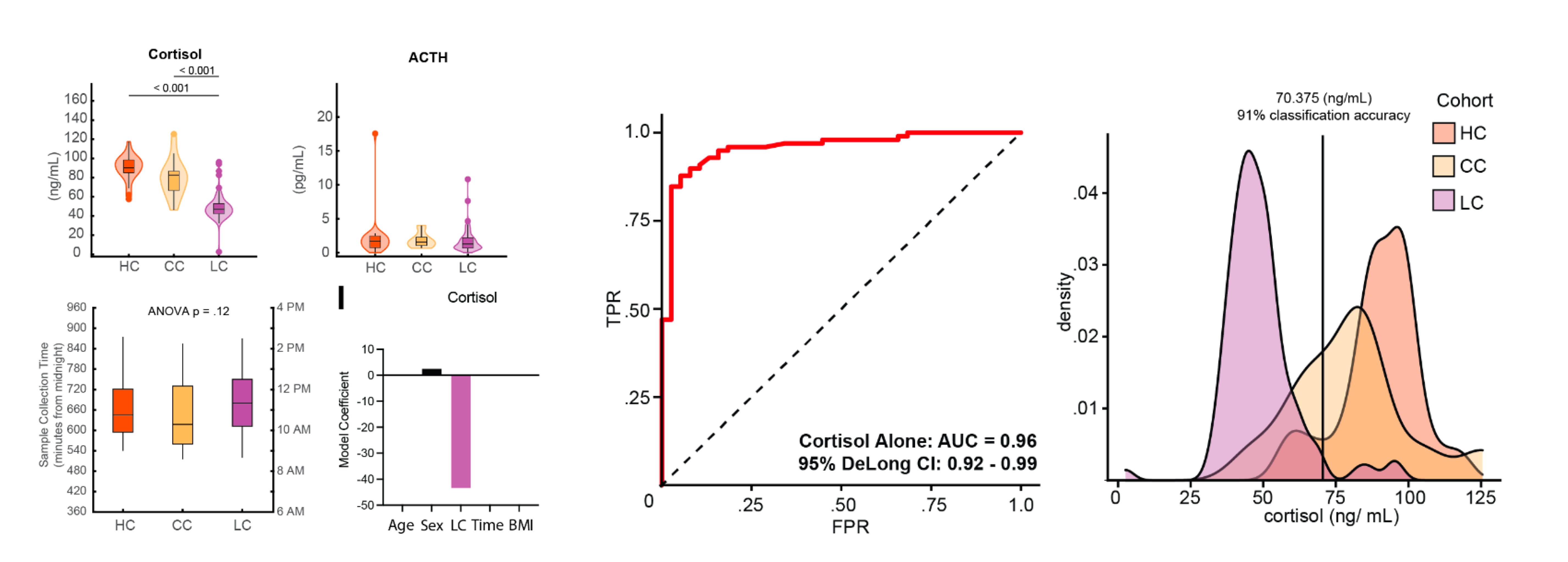
The cortisol and ACTH levels were drawn at approximately the same time in the different groups, which is important to note, since they are highly influenced by our circadian clock. The levels of cortisol were “uniformly low” among the people with Long Covid, as you can see from the partitioning in the far right diagram, and this marker was clearly the most significant predictor for Long Covid (an AUC of 0.96 is pretty striking).
ACTH should increase if cortisol is low, but it didn’t, which tells us the Long Covid individuals have a hypothalamic-pituitary-adrenal axis (HPA) dysfunction. Low cortisol has been noted previously with chronic fatigue syndrome (ME/CFS) but this is the first report to reinforce its potential importance as an underpinning of Long Covid. The stress that Long Covid symptoms induce, with persistent immune system activation in many, would be expected to increase cortisol levels. Their low levels can be linked to many of the well described Long Covid symptoms. But the basis for HPA dysfunction is unclear. Is it part of the neuroinflammatory process that can be a sequelae of a Covid infection? Direct involvement of the pituitary from Covid has been documented in case reports of pituitary apoplexy. A recent essay speculated on the potential of adrenal gland insufficiency but the lack of the pituitary-derived ACTH would suggest that would be secondary. While empiric steroids have been given to many patients suffering Long Covid without clear benefit, there would also be the risk of steroid use, per se, especially when given for prolonged duration, along with suppression of the immune response. Plus that would not get to the underlying HPA source of the problem. Of course, this important finding requires independent replication but, at the least, it may help to lay the foundation for a biomarker, if not provide a clue towards an effective treatment. Which gets us to treatments.
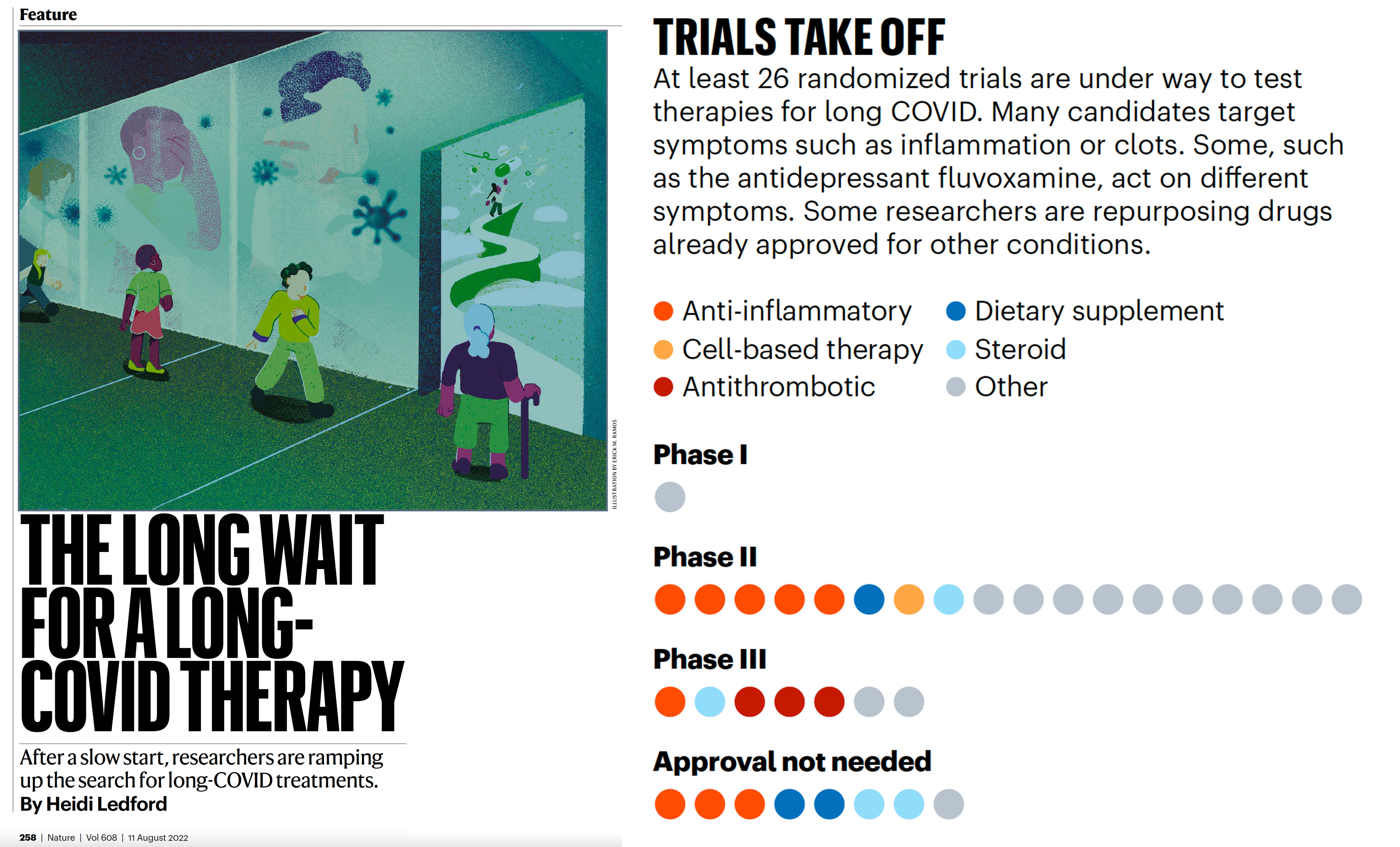
Treatments
These were reviewed in a feature at Nature this week by Heidi Ledford. You can see there were 26 different randomized trials that she was able to find, which included a potpourri of steroids, other anti-inflammatory agents, cell-based therapies, anti-clotting drugs, dietary supplements, and a big category of “other.” First, to emphasize that we have no therapies for Long Covid that have been validated. Second, all of these trials are quite small and disproportionate to the tens of millions of people who are suffering from Long Covid right now. So even if one of these trials “hits” with positive results, it will require a much larger trial to confirm potential benefit. Third, the trials are largely not being conducted on a cluster-specific basis, that is partitioning potential therapies to people with immune dysfunction symptoms as compared with those having predominantly dysautonomia symptoms (such as rapid and extreme increase in heart rate with standing). There likely needs to be very precise matching of a putative treatment with the symptom complex of the cohort studies, since Long Covid is a mosaic that include of both immune system and autonomic nervous system dysregulation.
The most heavily funded research effort for Long Covid is the NIH RECOVER project with $1.15 billion of support, but unfortunately it has been slow to test any treatments, which needs to be done rapidly and at scale when pilot results are encouraging. It’s great that there are so many randomized trials being done by other groups, but we are not nearly as far along as we need to be for zooming in on an effective treatment. And there’s interaction with validation of biomarker(s), since that might provide an objective metric for a treatment’s impact.
In summary, much new information for Long Covid was reported in a matter of days. It would be great to keep up this momentum, now that we are pushing onto 3 years of the pandemic. I have many colleagues who have been severely affected, and have seen multiple patients in my clinic in recent weeks who are debilitated. I wish I had something to offer them, but hopefully over time we’ll build on this recent spurt of knowledge. While we have no treatment or biomarker, the CDC relaxation of Covid guidelines is totally unhelpful— staying Covid cautious is the right move, and we desperately need better tools to block infections and transmission. There’s some hope that the first completed 4,000 participant nasal vaccine randomized trial could be the start of patching up the leak of vaccines against the Omicron subvariants (currently BA.5). Prof Iwasaki and I have called for an urgent Operation Nasal Vaccine initiative. There’s only one surefire way to prevent Long Covid: not to get Covid.