


Towards Solving the Long Covid Puzzle
A big week of new data and enhanced understanding
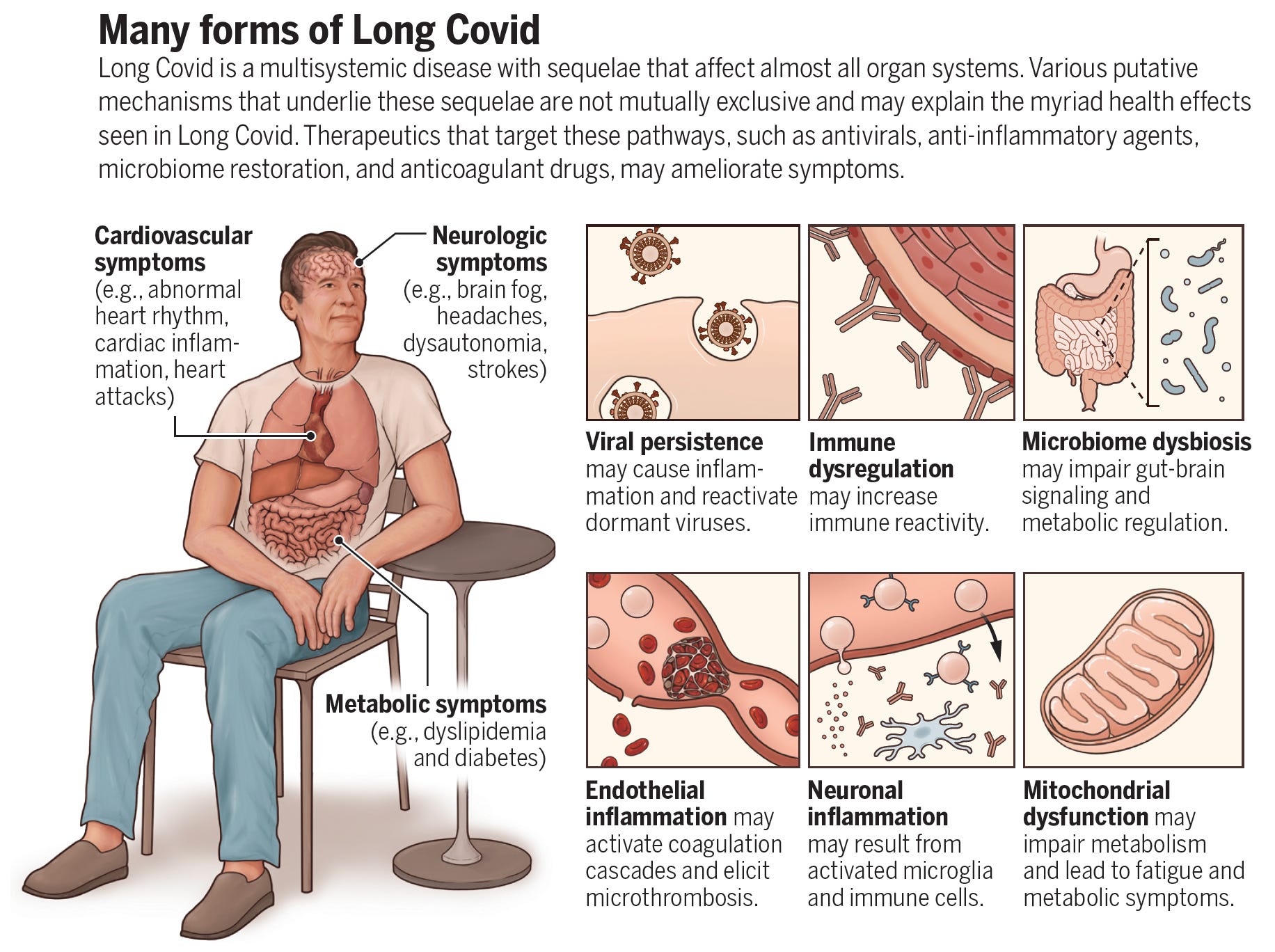
In recent days, there were several important new reports that help explain the pathophysiology of Long Covid. By coincidence, we published a Perspective in Science today to summarize the progress that has been made and the vital work that lies ahead.
Here we’ll summarize the new findings:
The Leaky Blood-Brain Barrier
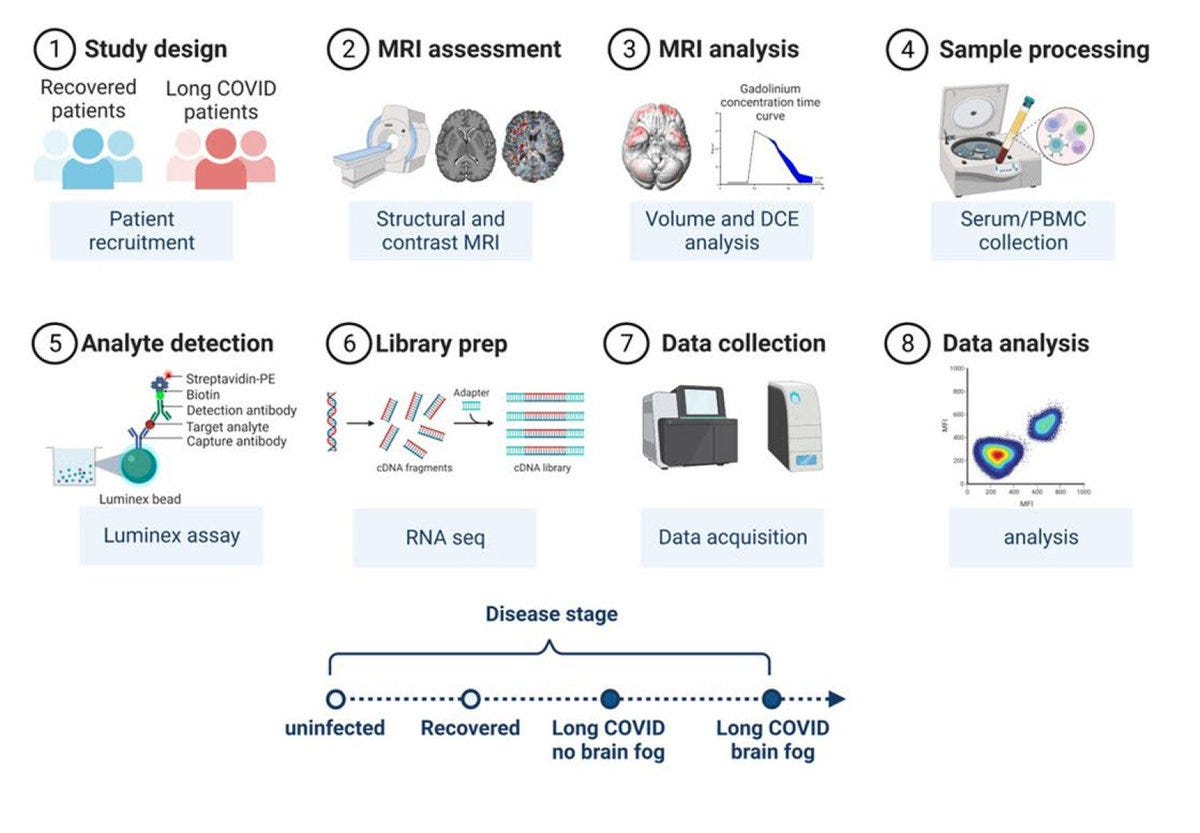
A systematic study of people with Long Covid and controls, using MRI, brain-specific S100β protein, RNA-seq of white blood cells, endothelial cell response in culture provided new insights about the disrupted blood-brain barrier (BBB) in individuals with Long Covid and symptoms of brain fog . They are well summarized by Prof Katerina Akassoglou from the Gladstone Institute who was not involved in the study and is a highly regarded scientist in the field of neurovascular inflammation: “This study is the first report of BBB disruption correlating with brain fog in patients with long COVID by dynamic contrast enhanced MRI. The MRI findings are in line with neuropathology reporting blood protein accumulation in brains from patients with COVID-19, and I expect that it will be the foundation for future studies at the blood–brain and immune interface for the discovery of mechanisms, biomarkers and therapies for neurological manifestations in long COVID.”
The numbers of participants in each group was small but the phenotyping was extraordinarily deep. Beyond the BBB, the notable findings were dysregulation of the clotting system and pro-inflammatory effects of endothelial cells.
Persistent Infections of SARS-CoV-2 as a Risk Factor
From a large community surveillance project in the UK , 381 participants were found to have evidence of persistent infections of SARS-CoV-2 for 30 days or more. That was considerably higher than anticipated.
1 to 3% had persistent infections for more than 30 days
0.1 to 0.5% had persistent infections for more than 60 days
Serial assessment of viral loads indicated many of the people had rebounding high levels, indicating there was likely actively replicating virus
The risk of Long Covid was 55% increased in people with 12 weeks or more of persistent infection, 24% increased in those with 26 weeks or more (adjusted odds ratio, Table below)

Interferon-Gamma As a Possible Biomarker for Diagnosis and Treatment
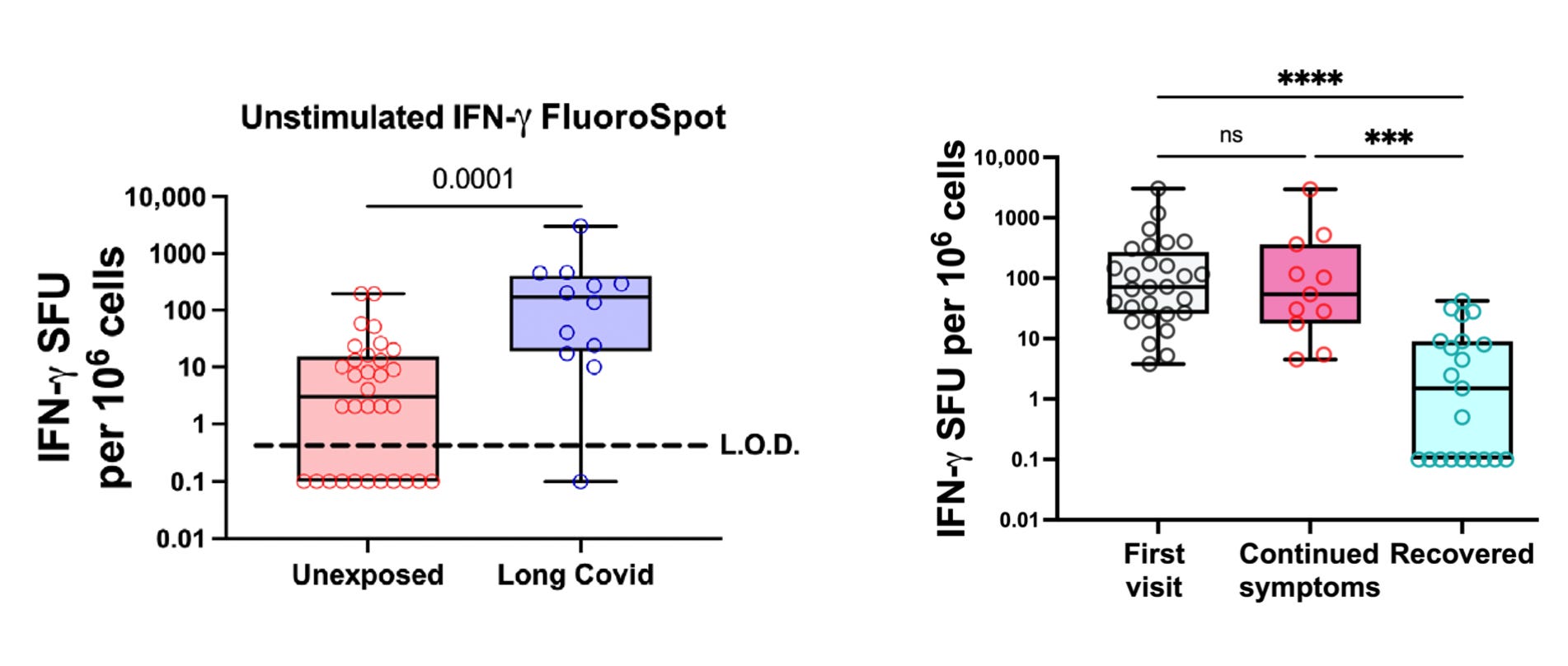
A new report assayed interferon-gamma, part of the first line of defense of innate immunity to a SARS-CoV-2 infection. Individuals with Long Covid had persistent elevation after the acute phase, and during follow-up serial assessment of this biomarker showed resolution among the participants with symptom resolution. This will need further assessment, but if replicated and extended, it might fulfill a major unmet need for both confirmation of diagnosis and a surrogate measure for treatments that are being assessed in prospective clinical trials, no less an objective metric for correlation with symptoms.
Myalgic Encephalomyelitis (ME/CFS) Deep Phenotyping
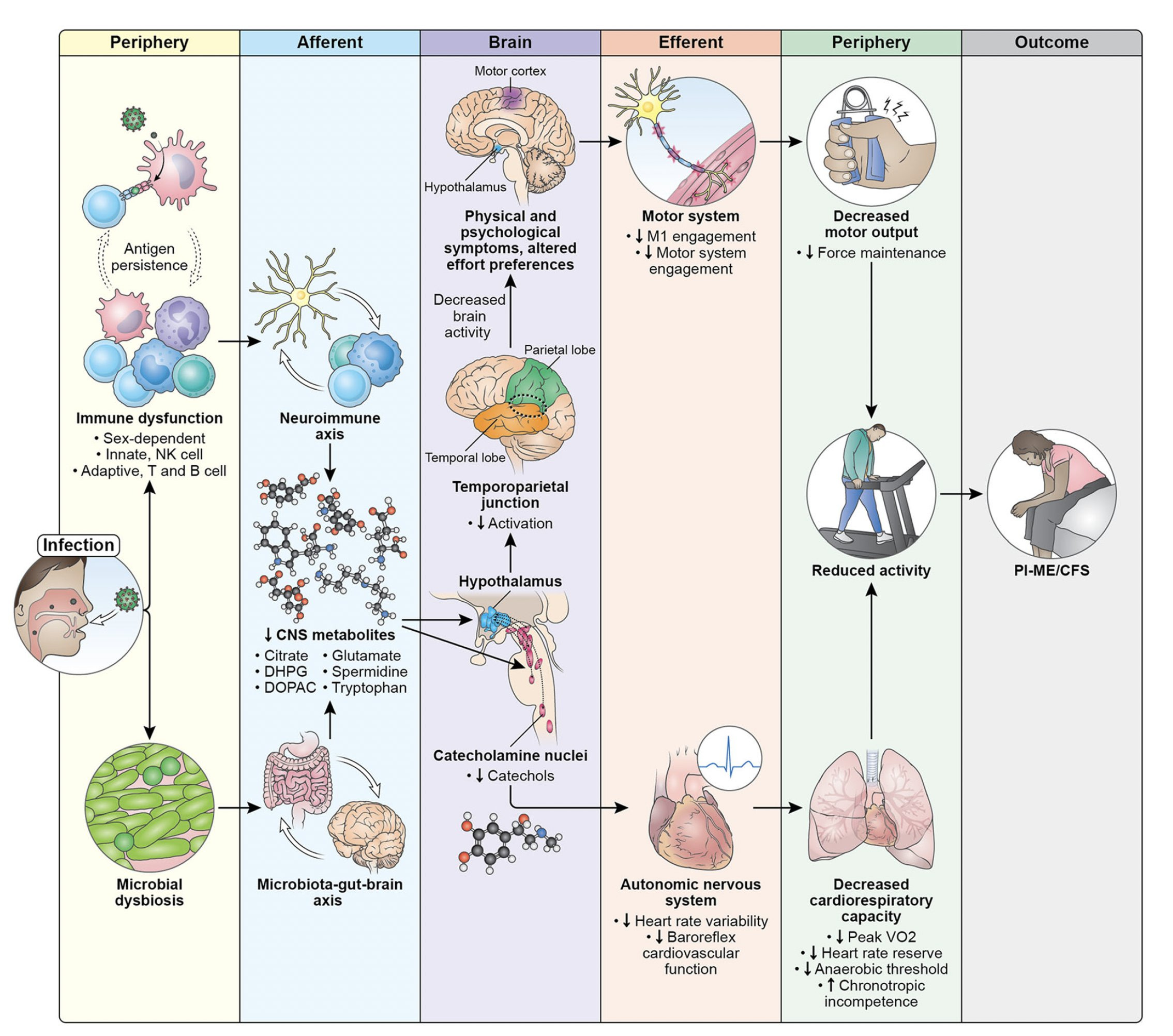
The 8-year, long awaited NIH project results were published in a 70-page manuscript. Like the BBB study above, the number of participants studies were small, but compensated by extensive characterization and suitable matched controls. With the considerable overlap of many of the symptoms of ME/CFS and Long Covid, the results are notable: signs of persistent chronic antigen stimulation with immune system dysregulation (with T cell exhaustion) along with multi-system disruption, some of which is central nervous system regulated, with specific regions of the brain implicated, and overall summarized in the graphic below.
On a related note, The Economist today had an article about post-infectious neurologic syndrome (PINS) that occurs with Covid, ME/CFS, Lyme, and several other viruses. “Michelle Monje, a neuro-oncologist at Stanford School of Medicine, homed in on precisely how covid-induced neurological damage might occur—particularly focusing on glial cells, as brain cells other than neurons are known.”
Prof Monje has just recorded a new Ground Truths podcast on this topic which will be posted very soon.
Two New Reports of Vaccination Protection Vs Long Covid
From a study in the Annals of Epidemiology, Michiganders derived an important protective benefit against Long Covid: Long COVID prevalence was 40-60% lower among adults vaccinated (vs. unvaccinated) prior to their COVID-19. This level of protection is consistent with many recent reports and has not been emphasized enough regarding an added benefit of booster shots. The data were previously reviewed on Ground Truths here.
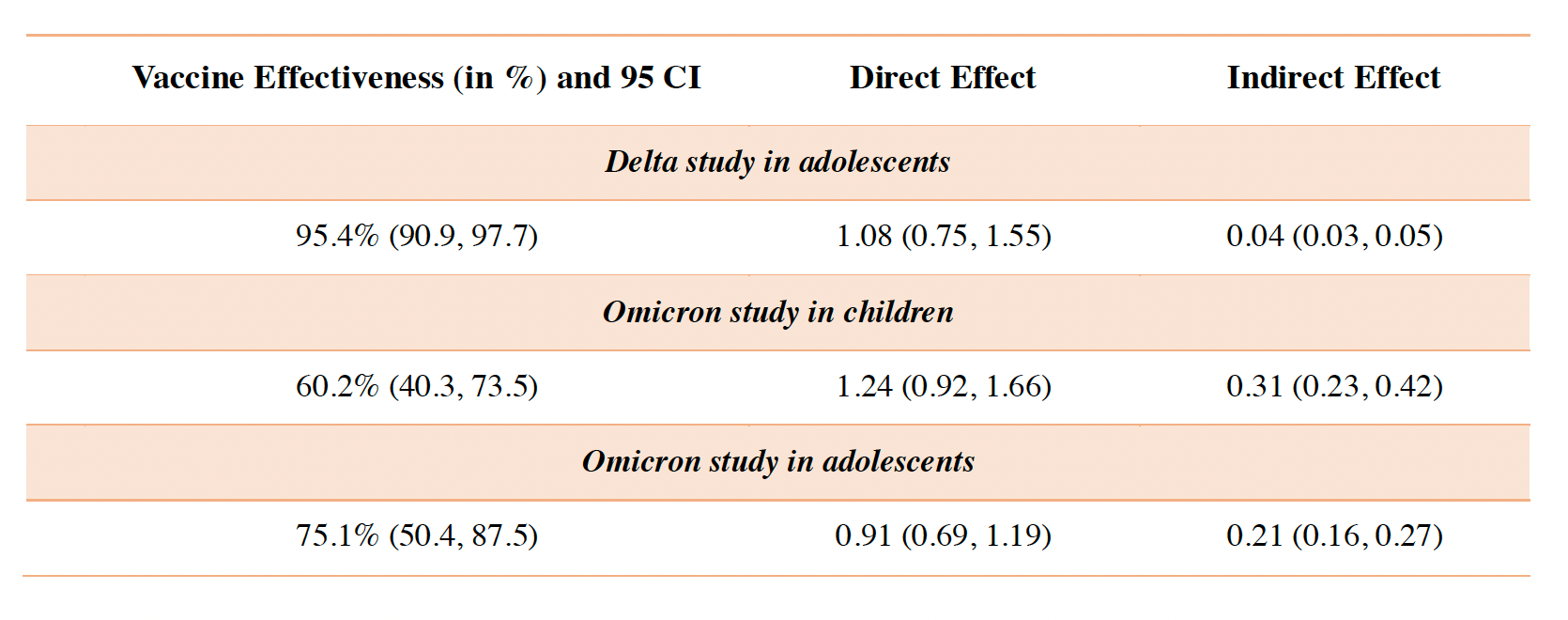
And a new preprint report on protection in children and adolescents which looked at different variants (Delta and Omicron) and cause and effect relationship for direct benefit of vaccination, summarized in the Table below. More protection was found in teens than children with the range of 60 to 75%.
Our Science Perspective
And finally, our essay in Science, in which we tried to encapsulate a lot of information on what has been learned so far, and what is desperately needed o be done now. Ziyad put together a great thread that reviews the key points
A little sample of some of those are below
A Brief Summary
We’re making considerable headway on understanding what drives Long Covid, along with the possibility of another biomarker candidate, which would be a big help as randomized clinical trials move forward. Clearly finding effective and safe treatments is an urgent matter and not enough is being done to pursue that yet, despite a long list of potential alluring interventions based on mechanistic insights. Hopefully that will get going now—it cannot happen soon enough.
Thanks for reading and subscribing to Ground Truths!
Please share if you found this post helpful
 | A guest post by
|
I hope this info is getting to the CDC as they are revising their Covid quarantine policy to cater to employers. Ironically, loosening the time frame will ultimately greatly diminish able workers.
In Dr. Michael Osterholm's most recent podcast, he cites a listener's experience in which a mother brought her Covid infected son to the ER (the infection had been confirmed). None of the medical personnel who treated him wore ANY type of mask, and they left the door open. The first place to start with prevention is in hospitals and clinics, but it seems even most doctors are no longer interested in this. Does the AMA have any position on this?