


When There is Actionable, Lifesaving Genetic Information
A new report shows some people unknowingly harbor genomic variants that could extend their lifespan 3-7 years
“By the age of 65 years, 10% of the participants with pathogenic or likely pathogenic variants in cancer genes had died. In contrast, in the group of participants without such a variant, 10% had died by 73 years of age.”—Plon and Jarvik NEJM, November 9, 2023
There have been several studies that have sequenced known disease-causing (pathogenic) genes over the years at the population level. Here’s a Table summarizing 4 of them, with the most recent being a unique study from Iceland.

Links for these 4 reports: Iceland, Geisinger, eMERGE, Oregon
As you can see from the Table, each of the studies sequenced a large number of people for a short list of known pathogenic genes and found that about 1 in 25 people harbored actionable genotypes that they didn’t know about. These reports date back to 2016, the first one coming from the large Geisinger health system in Pennsylvania, which, on the basis of their findings, went on to screen hundreds of thousands of patients and return their results. We’ll come back to returning their results later.
Before getting into the new report from Iceland, let’s go through some background.
Known Pathogenic Variants
Back a decade ago the American College of Medical Genetics and Genomics (ACMG) put together a list of actionable, medically important genes. Over time it has grown to the latest version of variants in 83 genes that ACMG recommends reporting because they are considered pathogenic or likely pathogenic (P/LP). Recall that this is out of about 20,000 genes in our genome, so it’s a tiny subset where the evidence is quite strong that there’s risk and something can be done to reduce the risk. Of that list, the CDC has identified 10 genes it calls “Tier 1” which consists of disease causing variants for hereditary breast and ovarian cancer, Lynch syndrome and familial hypercholesterolemia. There are approximately 2 million people who have these pathogenic variants in the United States but 90% don’t know they are affected. And that’s just 10 genes on the CDC list!.
The Icelandic Report
The DeCode Genetics group presented their findings for 73 genes (comprising the ACMG 2021 list) of the current ACMG list of 83 for nearly 58,000 people who were sequenced and over 108,000 people (note that the country’s total population is ~375,000) with genomic chip data who were, on average, born in 1960. The new, new thing here is that Iceland had the first established association of genomic data with lifespan data—something we have never seen before. So now we’re looking at not just actionable “pathogenic variants” but what can be considered potentially lifesaving genomic data. While many genomic variants might reduce morbidity (example: kidney stones), these are ones that are linked to changes in lifespan.
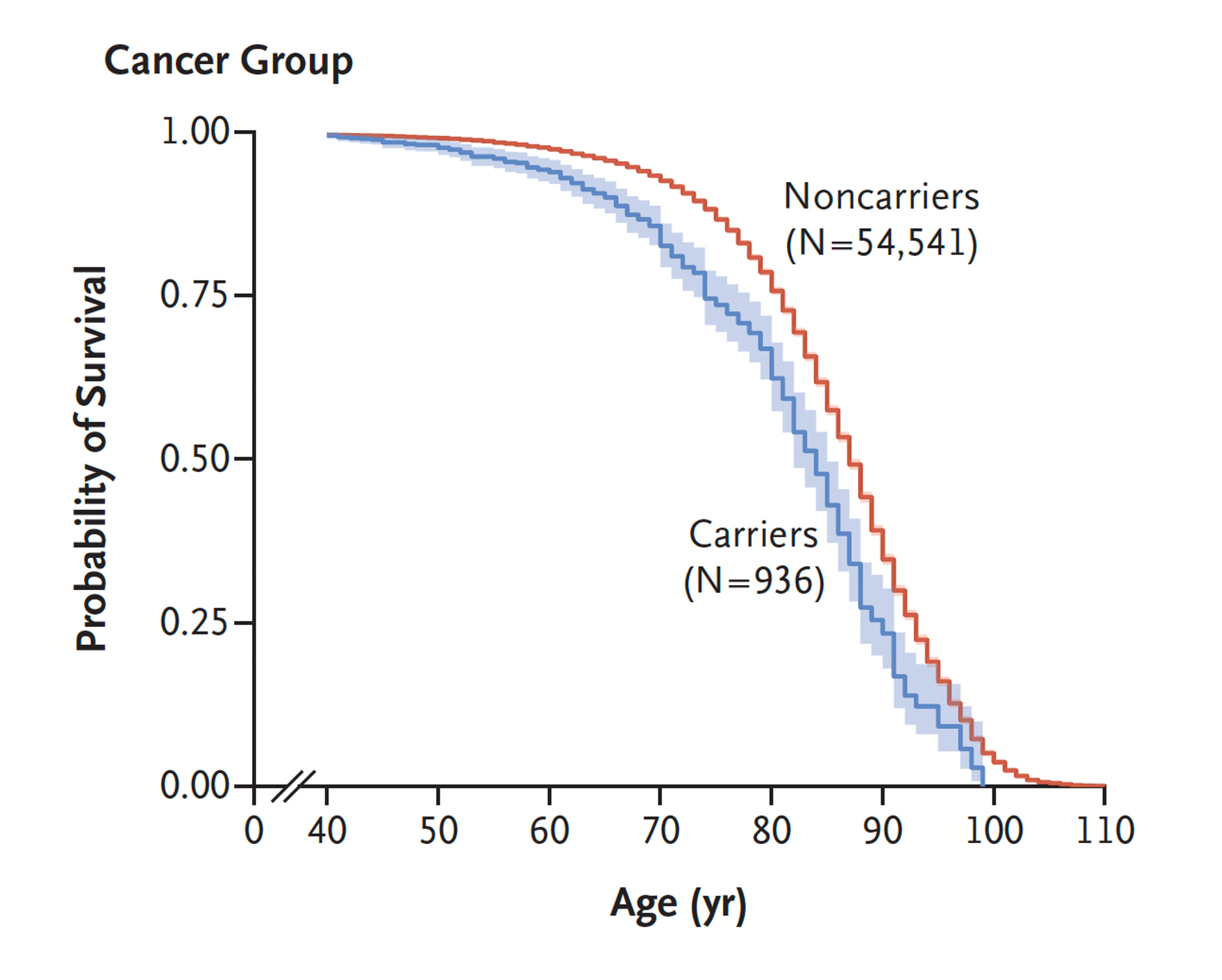
The cancer group of P/LP variants had the most pronounced association with lifespan, as seen below, and holding up to exclusion of a founder gene in BRCA2 in the Icelandic population. The average life span difference for these carriers of cancer variants was a 3-year reduction.
It wasn’t just cancer genes that had a significant association with lifespan, as seen in the Table below, as tied with the Icelandic Death Registry. Note in the “effect on life span” column, people carrying the LDL cholesterol receptor gene variant had 6.5 years of reduced life span (with 95% confidence intervals). Another cardiovascular gene variant in MYBPC3, which is an underpinning of hypertrophic cardiomyopathy, had a 2-year shortened lifespan. Of note, 42 individuals had more than one variant linked to lifespan reduction.

It is important to underscore that knowledge of these pathogenic variants are not just “actionable” but can be lifespan expanding, such that with cancer early and frequent screening can be undertaken (or prophylactic surgery when deemed appropriate), or with the cardiovascular genes (LDLR and MYBPC3) very aggressive treatment for cholesterol lowering or treatment for hypertrophic cardiomyopathy, respectively, would be expected to extend survival.
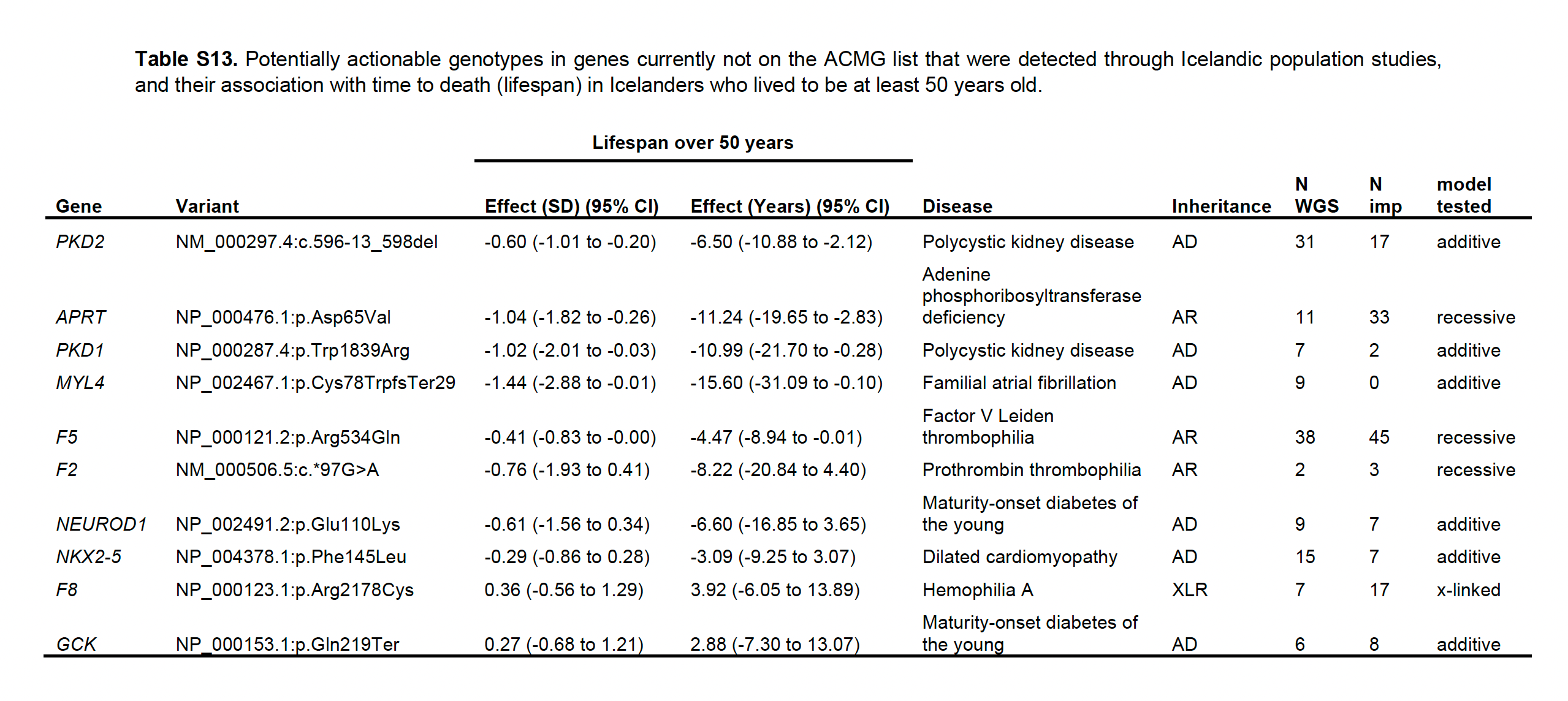
Beyond the ACMG list, the new report identified 10 more genes (Table below) that would be considered suitable additions to the list linked to kidney disease, blood clotting conditions (such as Factor V Leiden), hemophilia, atrial fibrillation, cardiomyopathy, and maturity-onset diabetes of the young (MODY).
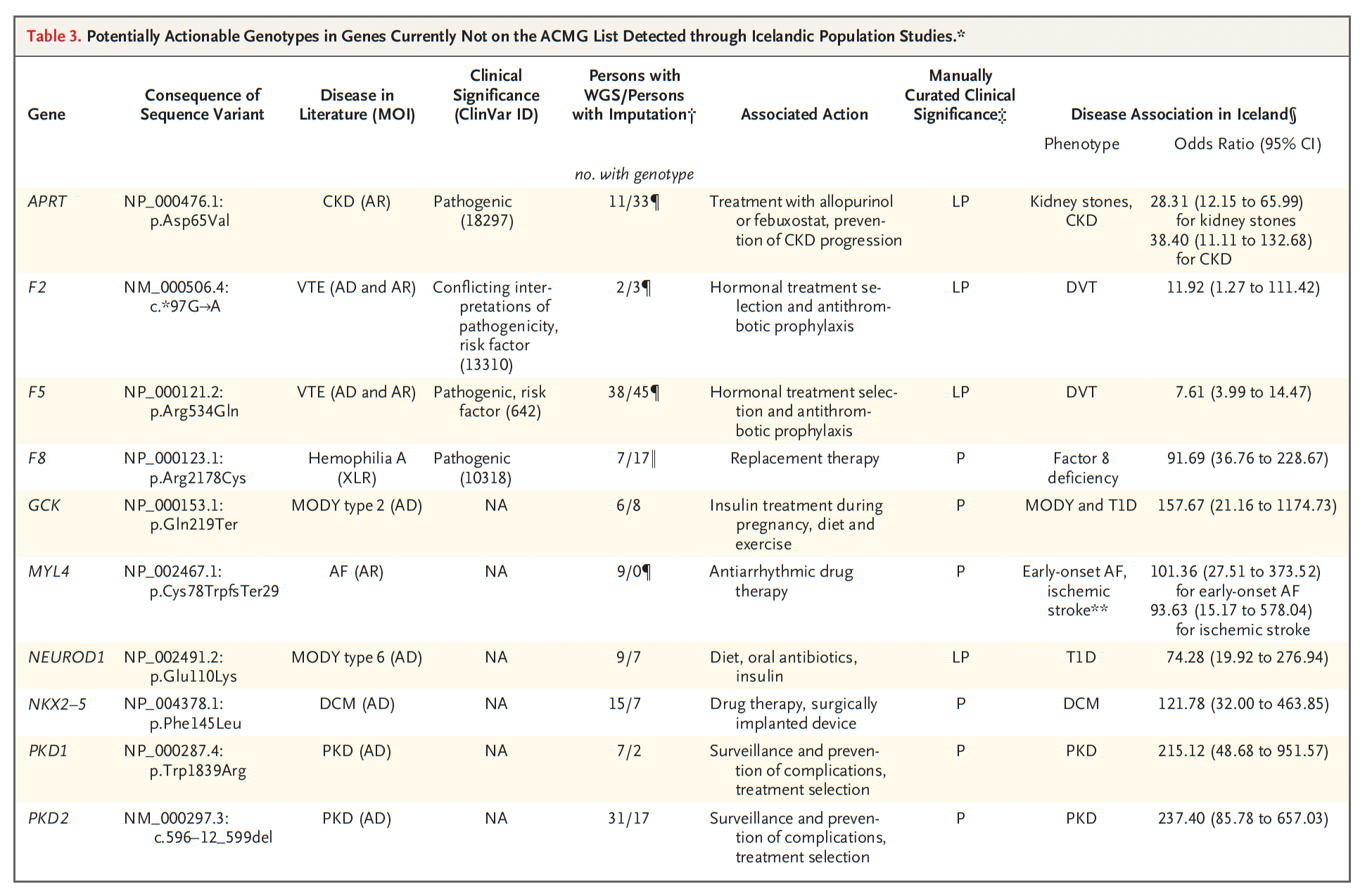
Many of these gene variants identified, while not linked with reduced lifespan, were associated with significant morbidity (Table below). Take a look at APRT and a 28-fold risk of kidney stones and 38-fold risk of chronic kidney disease, which can be prevented by taking allopurinol or febuxostat. The atrial fibrillation MYL4 variant had an odds ratio > 100 and an embolic stroke ratio of 94-fold. Dilated cardiomyopathy was strongly associated with the NKX2-5 variant (odds ratio of 122). There’s also polycystic kidney disease (PKD1 and PKD2 below with whopping odds ratios, yes with wide 95% confidence intervals. The list below doesn't include hereditary hemochromatosis (such as the HFE C282Y homozygous genotype) with adverse outcomes of cirrhosis and liver cancer that can be averted by frequent blood draws (phlebotomies). The authors emphasized the importance of detailed manual curation of the gene variants which increased the number of P/LP variants by 40%.
The Implications
The UK Biobank has genomic data for 500,000 people and the authors of the new report commented that the UK population has a similar frequency of variants as was found in the Icelandic population. This is important for 3 reasons. First, in all of the many seminal genomic studies published from the Icelandics to date, subsequent work has replicated their findings in people of European ancestry. So even with the one founder BRCA2 variant identified among Icelandics, all of the findings held up to its exclusion and with concordance of frequency in the UK population, that the association of 13 actionable gene variants with lifespan will likely be generalizable to people of European ancestry. Second, the new data from Iceland is based on a relatively small population and it is likely the number of genes associated with lifespan would be markedly increased with genome sequencing at scale and national death registry information. What is now 1 in 25 people with actionable lifespan-associated variants may well jump to 1 in 15 or 10 in the years ahead. Much more work needs to be done to identify the lifespan associated variants in multi-ancestry populations. Third, the UK Biobank does not return data to its participants. In the US All of Us study, nearly 300,000 participants have had their whole genome sequenced, but such data has not yet been returned to them.
This is a critical point that highlights the gap in genomic knowledge —now linked to lifespan—and willingness to share the data with the people who unknowingly harbor medically important variants. We have now crossed a line with the new study. We’re no longer referring to pathogenic variants, but ones that can substantially alter a person’s lifespan. Only 2 countries around the world offer their population sequencing: Israel for BRCA1 and 2 in the Ashkenazi population and Iceland for BRCA2. The CDC considers 10 genes “Tier 1” —most of which had a lifespan link in the new study—but is doing nothing in the United States to promote their ascertainment by the public.
Recently, Guzauskas and colleagues performed a modeling analysis for population screening of 3 of the CDC Tier 1 conditions (Hereditary breast and ovarian cancer, Lynch syndrome and Familial Hypercholesterolemia) and concluded it would be cost-effective in adults younger than 40 years if the genomic test was at a relatively low cost of $250 or for people 50 years old at $166 per test (summary for patients). We are now at that level whereby whole genome sequencing has dropped to the $200 threshold, and targeted sequencing or arrays can be done at substantially lower costs. It doesn’t appear that we can continue to use cost now as the reason to not obtain information that can be lifesaving.
Moreover, there are now millions of people who have had genome sequencing (exomes or whole genomes) but their data has not been returned to them. With the new report, can that be considered acceptable?
Thanks for reading, subscribing, and sharing Ground Truths!
All content from the Ground Truths newsletter posts and podcasts are free.
Any and all voluntary financial support goes to Scripps Research.
Disclosure: I was previously an advisor to Illumina, a genome sequencing company, but resigned earlier this year.

@Eric, Given the relatively low cost of sequencing, are there potential concerns for use of this information by health insurers to decline or alter coverage based on either running the the assay or discovering the information in the patient’s medical record? If so, are there any protective steps for the public to take?
An MD I visited not long ago proposed I get genetic testing. I had the sense that she was proposing this to all her patients, no matter their demographic (she had a flyer she was giving out to her patients). I am well into my golden years, with no offspring, so it didn’t make sense to me why she would propose it. For younger people, though, it definitely does seem worth considering. But this is all layperson conjecture, and it would be interesting to hear what you think about when it is most indicated to get this sort of testing.