


A break from Covid waves and a breakthrough for preventing Long Covid
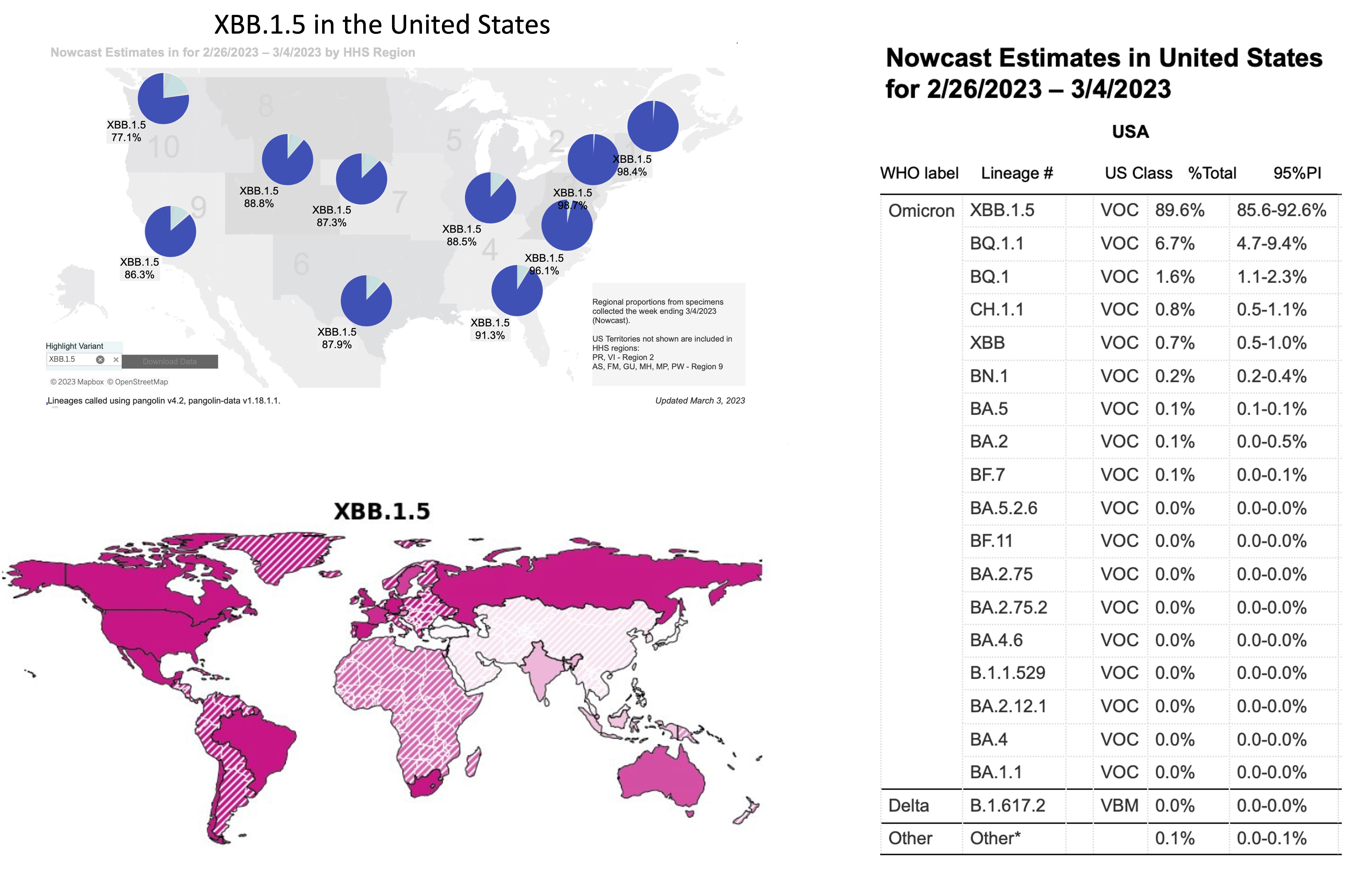
All indications from genomic surveillance of the virus, wastewater. and the clinical outcomes that are still being tracked (albeit more limited and less periodicity as time goes on), that we’ve (finally) entered an endemic phase (think smaller “wavelets”). There are no new SARS-CoV-2 variants that have yet cropped up with a growth advantage over XBB.1.5 (the recombinant with 2 significant mutations added on) which is dominant throughout much of the world, or its cousin, XBB.1.9.1. For all the talk about the convergent “variant soup” that preceded the most recent wave, the XBBs took hold and are not giving way to a long list of Omicron family sub-variants (Table below). Moreover, the XBB.1.5 variant ascent to dominance was not associated with a surge of Covid hospitalizations or deaths in the United States or elsewhere in the world, which might have been predicted based on its properties of enhanced transmissibility and immune evasiveness compared with earlier versions of Omicron.
We’ve been dealing with Omicron since November 2021, starting with BA.1 and marching through a number of its lineages (such as BA.2, BA.2.12.1, BA.5, BQ.1.1) over these 16+ months. It’s getting harder to think how further mutations added on to Omicron will pose a major threat, given how the population immunity wall that has been progressively built over 3 years—from infections, vaccination, boosters and their combinations— seems capable of fending off major waves vs this family of the SARS-CoV-2 virus. But there are 2 points of concern.
The High Baseline of Covid Hospitalizations and Deaths
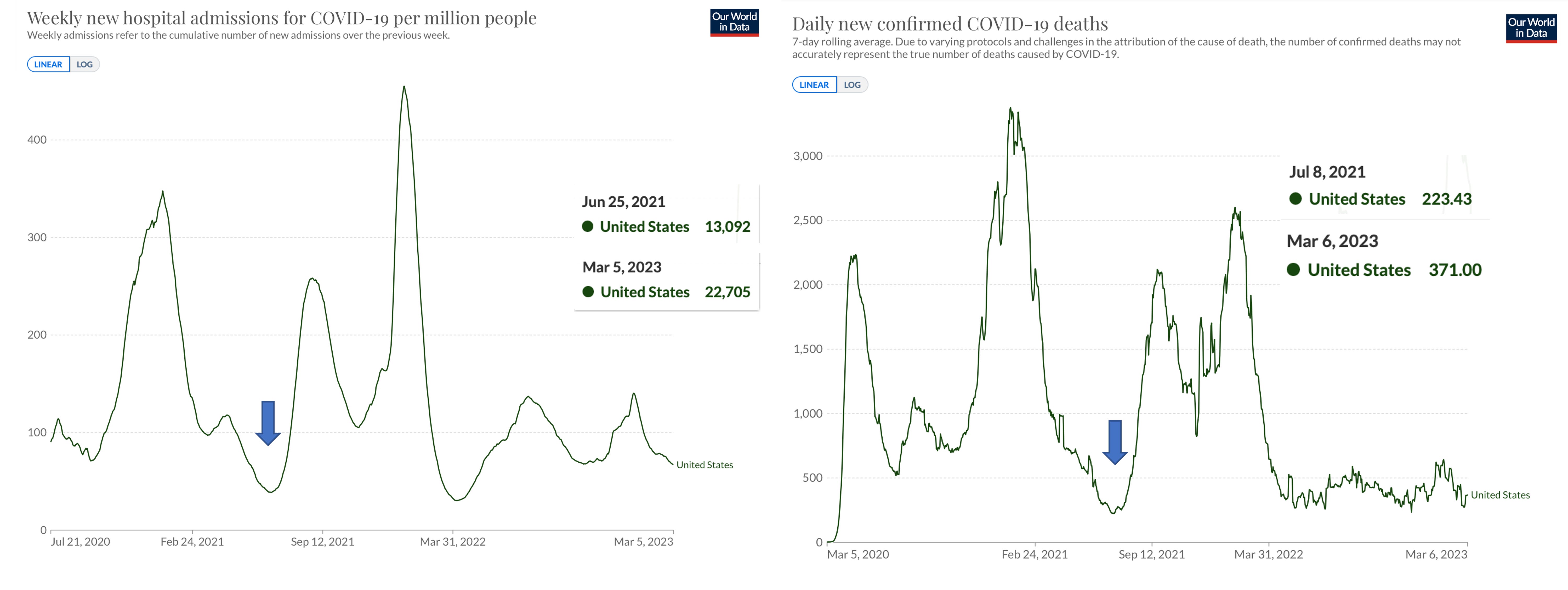
First, we sit at a very high baseline of daily Covid hospitalizations and deaths in the United States, over 25,000 and about 400, respectively. This is far beyond (double) where we were in June 2021, pre-Delta, when we got down to close to 10,000 hospitalizations and ~200 deaths per day. There’s still no shortage of circulating virus (currently XBB.1.5) getting people infected and some of the folks of advanced age and immunocompromised are the ones chiefly winding up with severe Covid. The virus is finding the vulnerable people more easily since their guard is let down, abandoning high-quality masks and other mitigations, and the low rate of keeping up with boosters in the last 6 months (the age 65+ rate is 40%). There are about 15% of Americans (more than what many people think or have been led to believe), based on all the serologic data available, who never had Covid and are relying on their vaccines/boosters to avoid their first infection. Reinfections among the 85% with prior Covid are not uncommon and not necessarily benign. No less, the pervasive attitude is the pandemic is over, life goes on. That’s helping the virus find new or repeat hosts.
That high baseline also shows up in the wastewater data, no where close to where we were in the Spring of 2021.
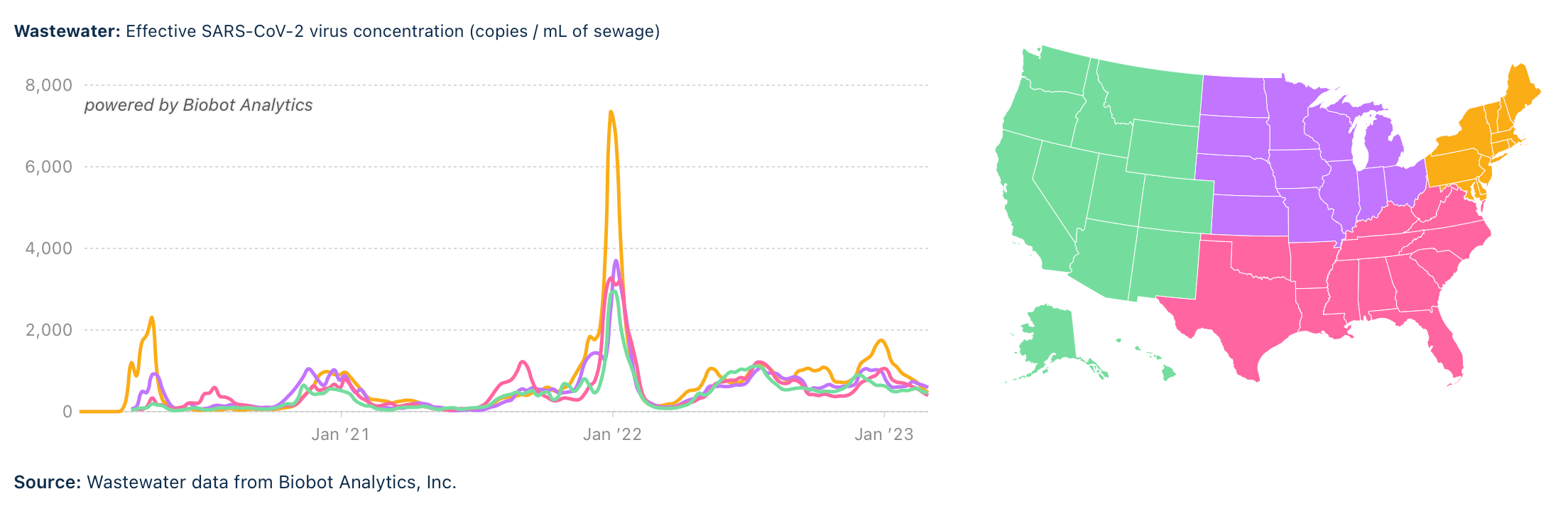
Which bespeaks the problem: SARS-CoV-2 is not in the rear view mirror, no matter how much that is wished or believe. Just that we may not see big surges of cases and adverse outcomes unless there is……..

Another “Omicron Event”
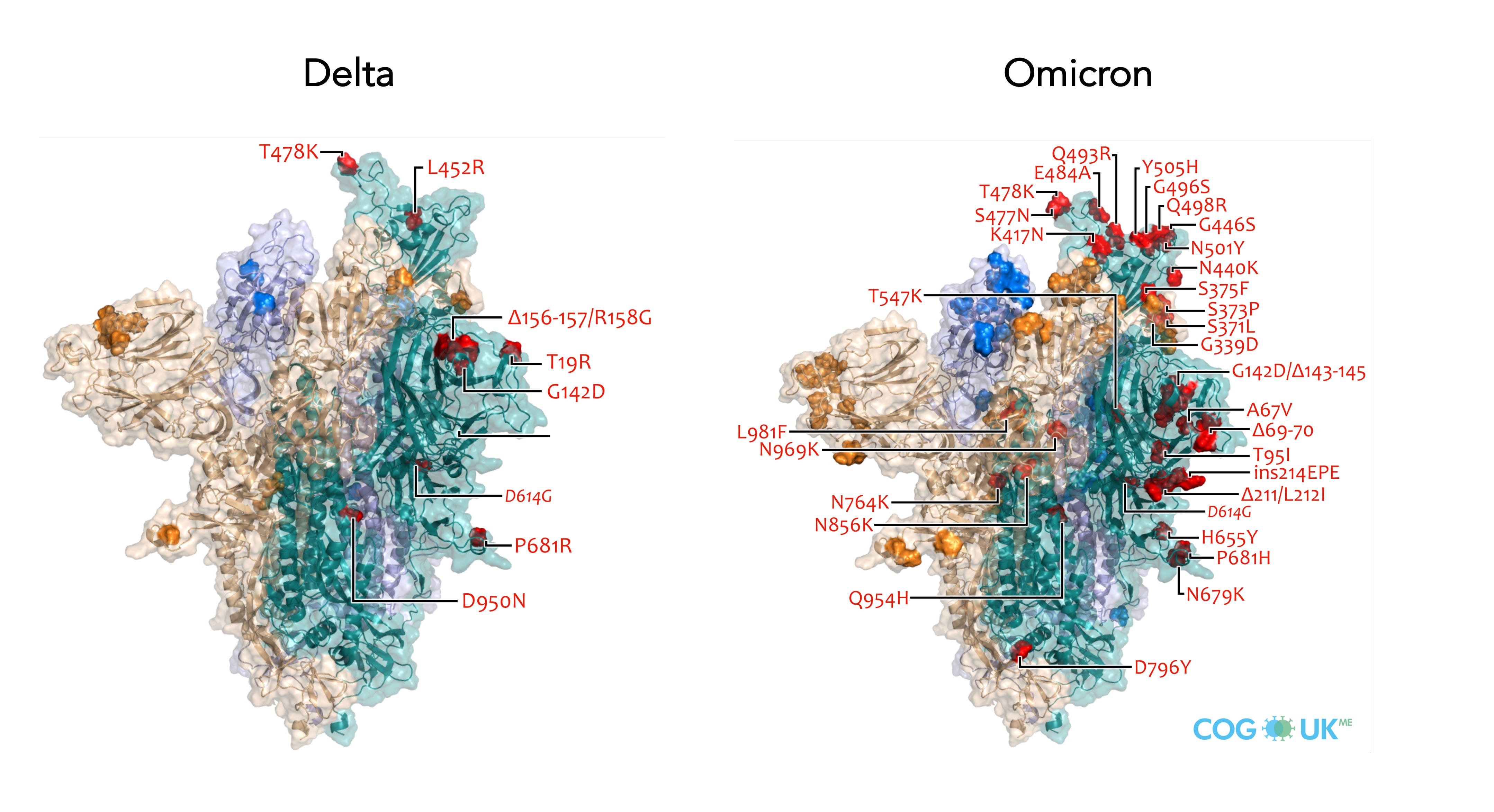
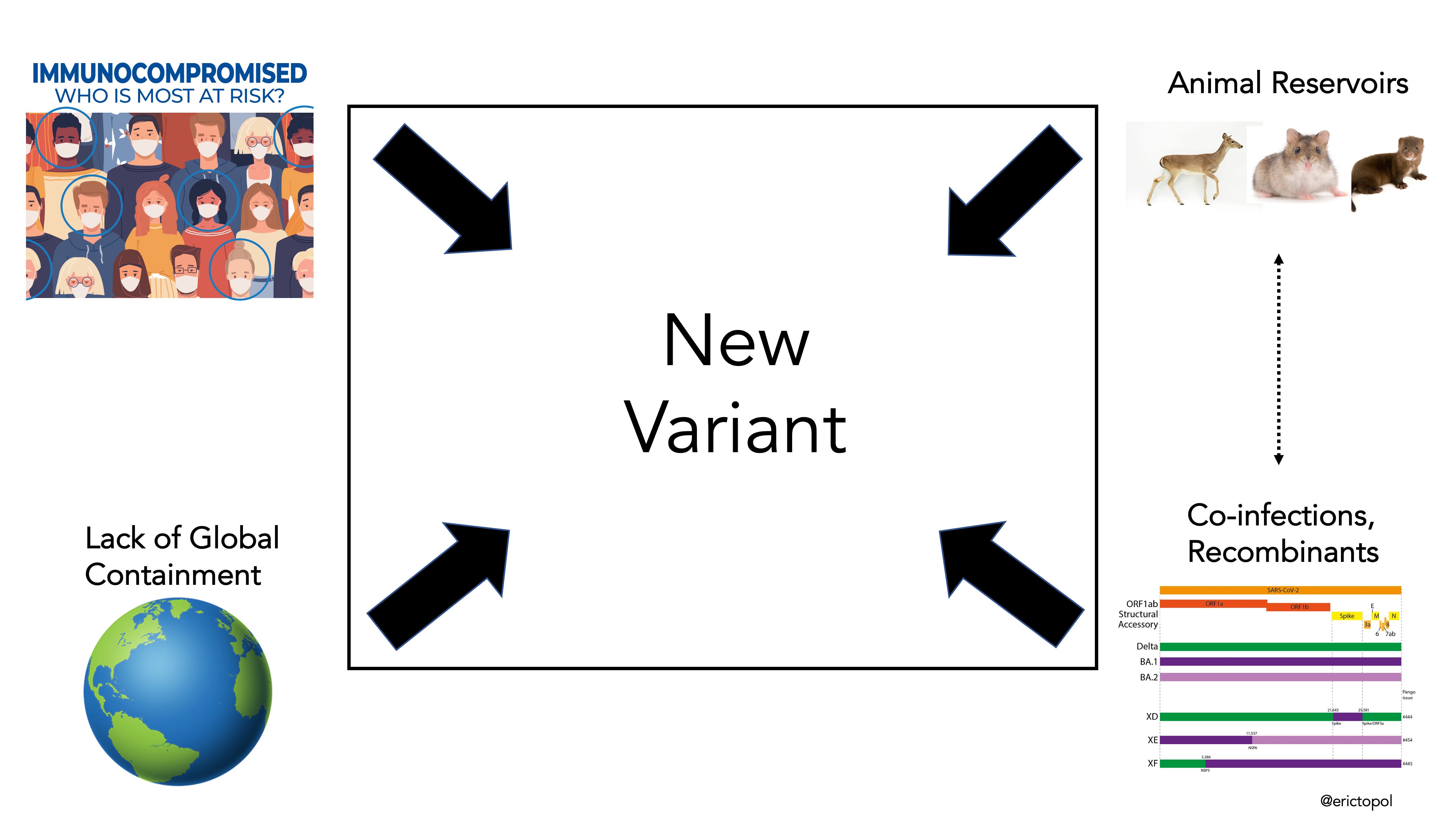
That brings me to the second concern, which is considerably more important. That we will or might see on “Omicron event.” This likely occurred from the hyper-accelerated evolution of the virus within an immunocompromised host that was then transmitted. Whether it’s via this path or others (graphic below), a new family of viruses, let’s say with the Greek letter designation of “Pi,” might show up that are distinct from BA.1, with a major growth advantage. So antigenically distant from our immune recognition system that Pi could present a serious challenge to our immunity wall, or might again be hyper-transmissible like Omicron BA.1, or potentially more virulent like Delta was compared with Alpha (or combinations of these 3 properties). Recall how there were over 50 new mutations in Omicron BA.1 compared with the ancestral strain. Take a look at all the changes compared with Delta, its major variant predecessor, (as shown in part by the spike protein mutation map below) and XBB.1.5 has considerably evolved, built on that further.

When 10 scientists who are following the pandemic and the virus evolution closely (including me) were recently asked what are the odds of another Omicron event in the next 2 years, the range was 5-30%, with no one thinking it is zero, and good convergence at the 10-20% level (unpublished data). And that’s in the 2-year window. SARS-CoV-2 will be with us for many years, so over time that likelihood forecast for a Pi new family of variants (and beyond Pi) increases. There are too many routes for us to see evolution of a Pi family of variants as shown in the graphic below. That is why we must prioritize development and validation of next generation vaccines that can achieve variant-proof protection (e.g. against all betacoronaviruses) and have improved defense against infection that can be accomplished via mucosal immunity with oral or nasal vaccines.
Now the good news.
A Breakthrough for Prevention of Long Covid
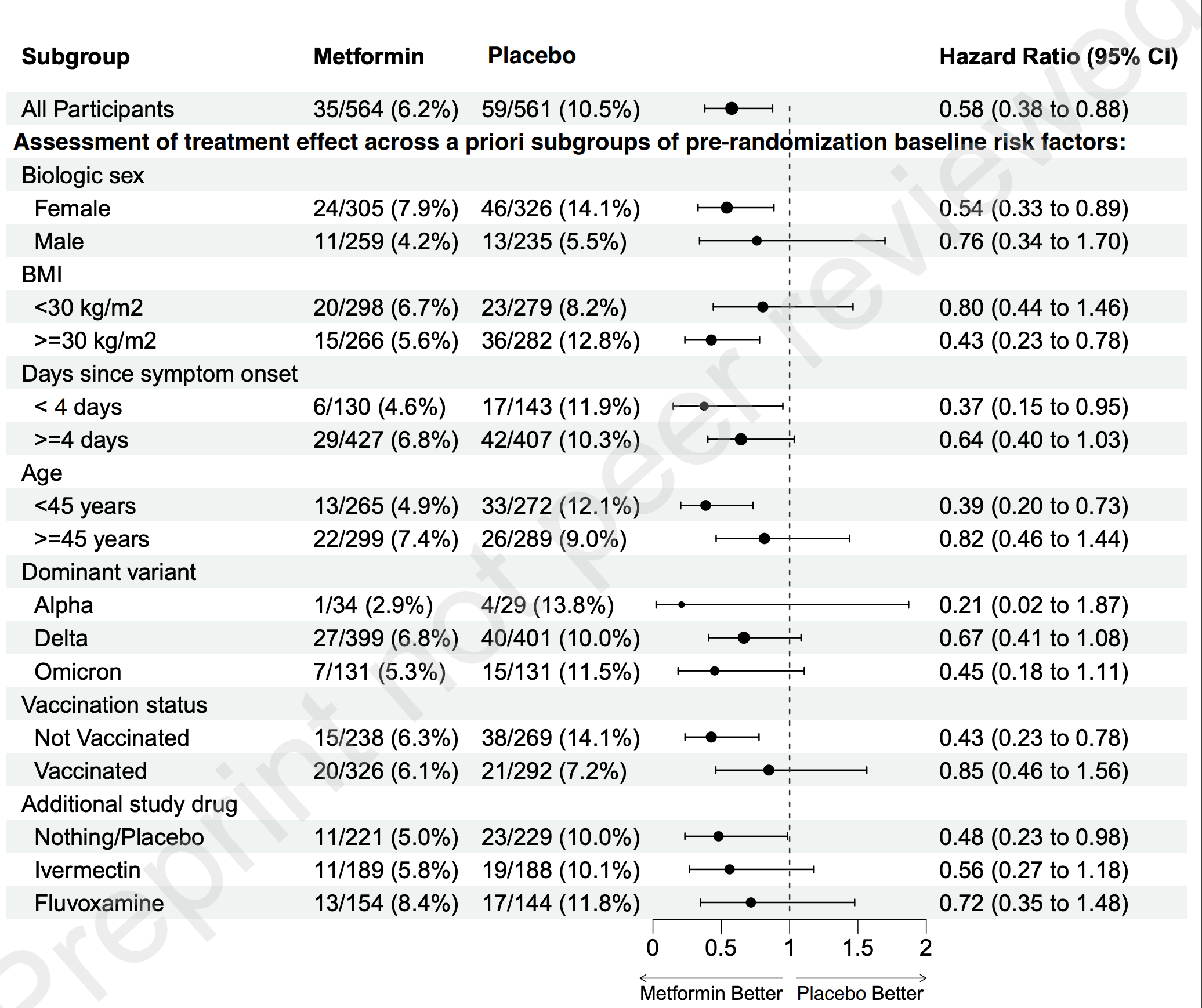
Until now the only way we knew that Long Covid could be prevented was to not get Covid. That’s still the case. But a new randomized, placebo-controlled trial of metformin has yielded exciting results—the first drug to be shown to help prevent Long Covid. Over a thousand people with mild-to-moderate Covid were randomly assigned to 2 weeks of metformin (500 mg pills, 1 on day 1, twice a day for 4 days, then 500 mg in AM and 1000 mg in PM for 9 days) or placebo. There was a 42% reduction of subsequent Long Covid as you can see by the event curve below, which corresponds to an absolute decrease of 4.3%, from 10.6% reduced to 6.3%.

Of note, the participants in the trial were fairly representative of the people who most often go on to manifest Long Covid, outpatients with a median age of 45 years and 56% were female. The low risk subgroups of people age <30 years or with a normal BMI were excluded. There were no treatment by subgroup interactions—that is there were overlapping 95% confidence intervals for the direction of benefit for metformin for all subgroups; no clear evidence that metformin worked better or worse for each. That’s consistency, although the statistical power for an interaction term is limited with only ~1,000 patients and a larger trial would be needed to know whether any of the subgroups below had differential effects with metformin. The findings in the trial also reinforced the higher risk of unvaccinated vs vaccinated status to get Long Covid (14 vs 7% , respectively, among placebo assignees). The diagnosis of Long Covid in the trial relied upon it being documented by a medical provider. The mechanism of metformin’s apparent benefit is unknown, but perhaps is related to its impact on reducing oxidant stress and inflammation, or suppressing viral replication, as has been demonstrated in the lab and in vivo models with the SARS-CoV-2 virus.
There are no other adequately sized or rigorous trials that have evaluated metformin to date. So the question is, without an independent replication, whether this trial’s data should be considered sufficient to now recommend metformin in clinical practice. My view is yes, since the risk of side effects for 2 weeks of metformin is near zero (from both the trial itself and the huge experience with metformin over decades for chronic use) and the cost is remarkably low, in fact as low as $1-2 dollars for the 2 week course. The only other drug to date with some promising data to prevent Long Covid is Paxlovid, but that is from a large observational database, not derived from a randomized trial. Ideally, a 2X 2 factorial design trial would be conducted to test metformin plus paxlovid, either drug alone, or placebo. And to emphasize, we still have no drug validated to treat Long Covid, only 1 that now appears likely to help prevent it.
As I’ve written in the past, I don’t use the term “breakthrough” lightly. Besides Paxlovid, that I initially wrote about in 2021 here, and the new anti-obesity drugs here, I’m reluctant to go there. But to see such a pronounced benefit in the current randomized trial of metformin, in the context of it being so safe and low cost, I’d give it a breakthrough categorization. Another way to put it, that unless or until there are data to the contrary, if I got Covid, I’d take metformin for 2 weeks at the doses used in this trial.
I hope you find this edition of Ground Truths useful. If you haven’t already, please subscribe (it’s free) and consider sharing. I plan to have less presence via twitter in the times ahead and will be using Substack more to get what I consider important new information out.