
The aphorism “You Are What You Eat,” with roots that date back to 1826, is a ground truth. Or we can go way back to what has been mis-attributed to Hippocrates: “Let food be thy medicine and medicine be thy food.” A systematic assessment across 195 countries concluded that a poor diet is linked to 22 per cent of all deaths, which accounts for more deaths globally than tobacco, cancer, hypertension or any other medical condition or health risk. So what is a healthy diet? There are about 40,000 diet books on Amazon which epitomizes the problem: the evidence is thin for what constitutes the optimal diet that promotes health, no less the notion that it should be the same for all people. Historically, “food science” can be considered an oxymoron because of its reliance on the notoriously inaccurate memory of study participants or their food diaries, lack of randomized trials that are extremely difficult to conduct, and heavy influence of the Big Food industry. The global diabesity epidemic has been fueled, at least in part, by our diet. Now that the GLP-1 drugs have come on the scene to treat diabetes and obesity, there’s irrational exuberance that we’ve solved the problem, and will be able to prevent the cardiovascular, metabolic, musculoskeletal, and neurodegenerative consequences.
In aggregate, several recent publications, two very popular books, and a new, large $189 million NIH clinical trial, may help to provide an objective basis for what we should eat to be and stay healthy. This could someday even lead to precision nutrition—the individualized diet that aligns best with each person’s multiple layers of data (such as metabolism, microbiome, physiology and genetics). I’ve read, written about, and interviewed the authors of the 2 books (Peter Attia’s here and here, Chris Van Tulleken here). In this edition of Ground Truths, I’m going to review a bit of what we know now about healthy and unhealthy food, and where we may be headed.
Here and Now
UPFs
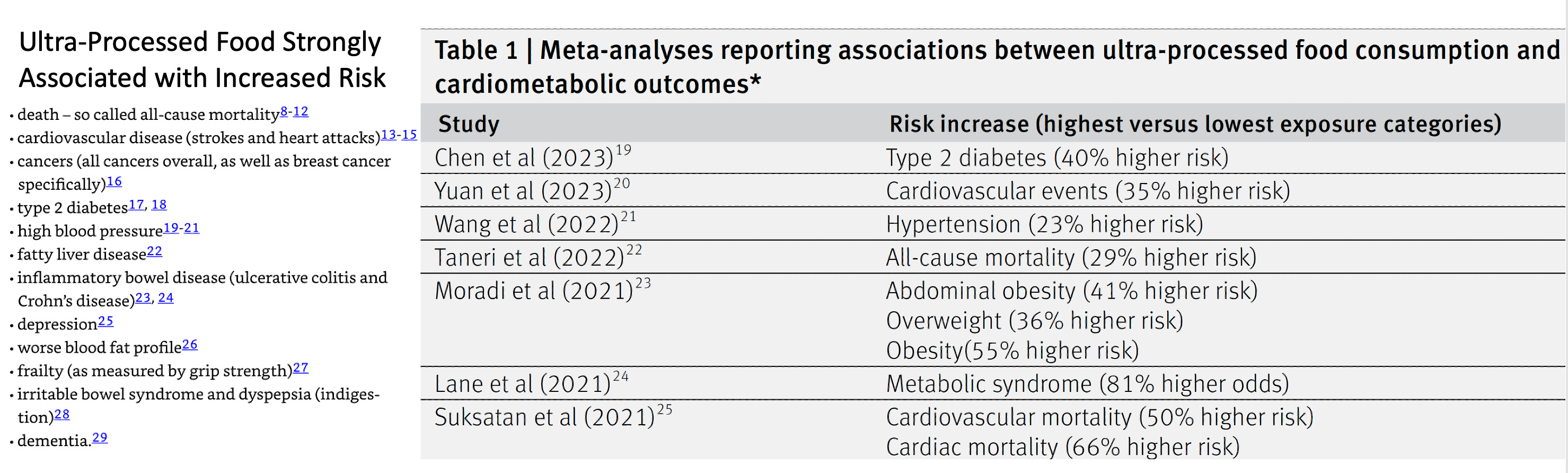
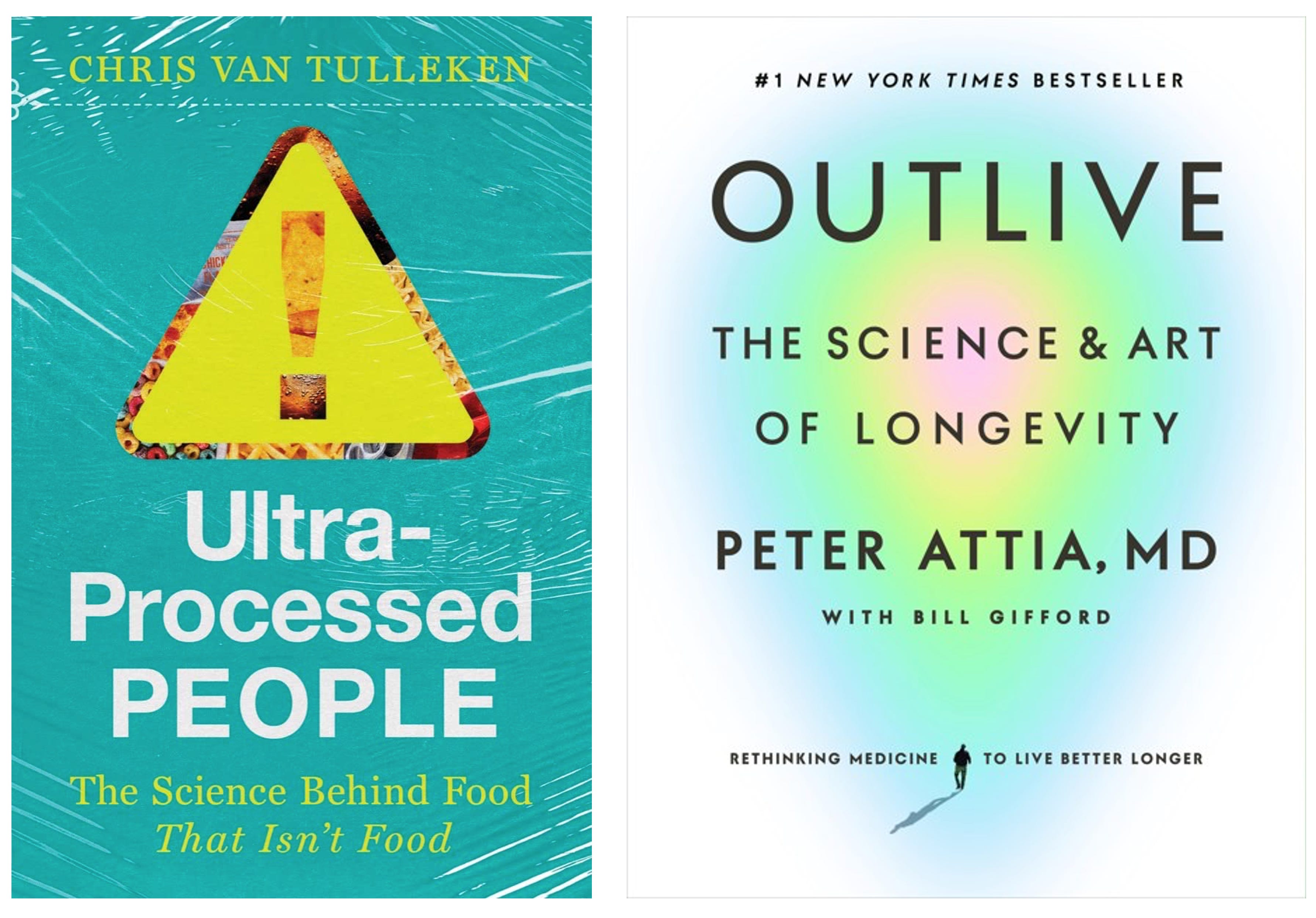
A very compelling case against ultra-processed foods (UPF) was made in Chris Van Tulleken’s book (left panel, below) and a recent BMJ review (right panel), as summarized in the Table below. When you review the 2 lists and the evidence that’s cited, it’s hard to believe that we’re not doing anything about it.
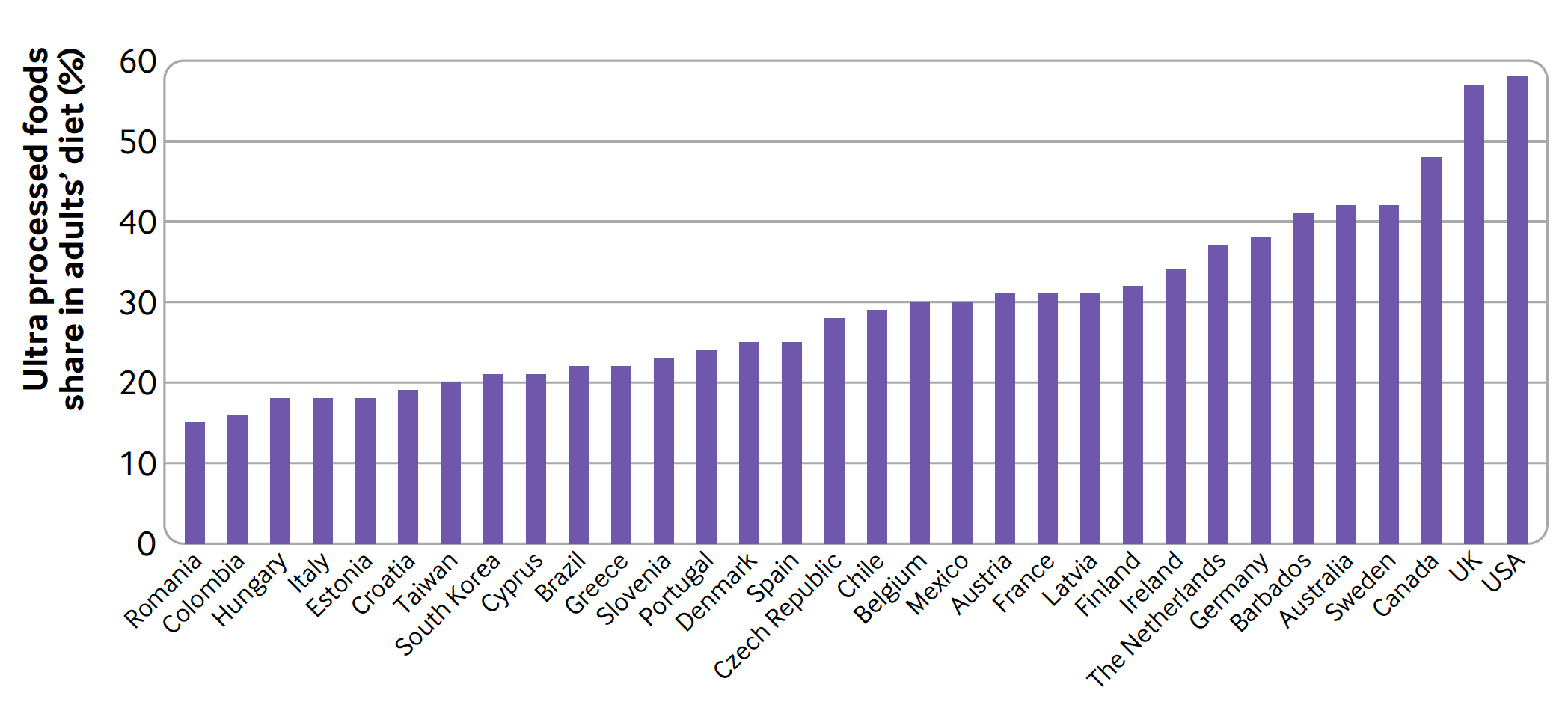
Especially when you consider that the USA leads the world at near 60% of its diet in adults that is UPF and in today’s print edition of the New York Times Magazine, Dr. Helen Ouyang pointed out that the diet in children is about 70% UPF. If you read what happened to Chris Van Tulleken after eating an 80% UPF diet for 1 month, with baseline and follow-up blood tests for inflammation and MRI brain scans, you’d be alarmed.
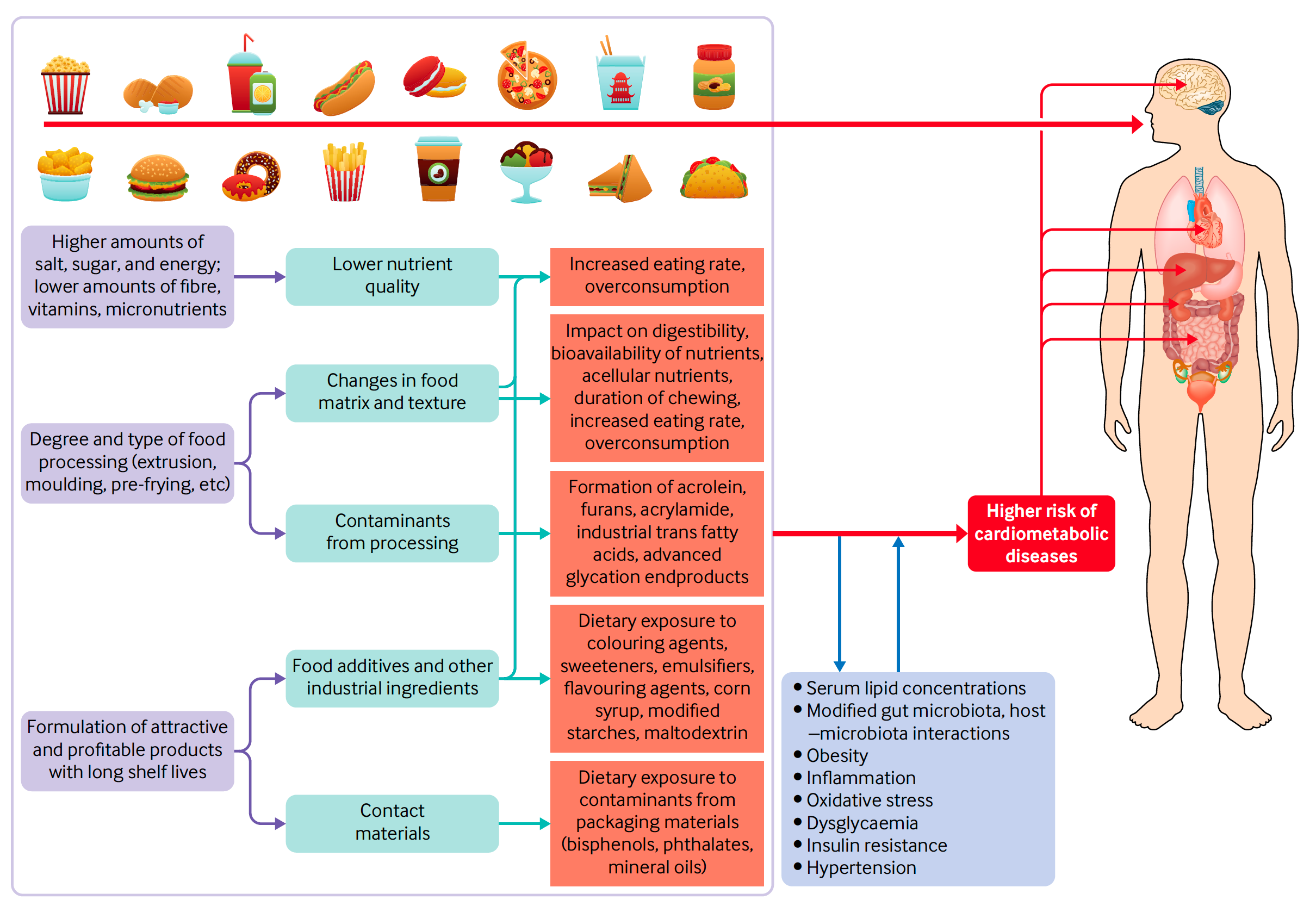
I think of the acronym UPF as like UFOs—foods that contain alien additives and preservatives, laced with sugars, salt and fats, that have been throughly tested by Big Food to be highly addictive, feeding our neuronal reward circuits. The U in UFOs that stands for unidentified is key—you’ll see them in the small print, long list of ingredients of foods, but they don’t show up in the readable nutrition label that is dedicated to macronutrient carbohydrate, protein and fat content. Furthermore, as Chris Van Tulleken defined UPFs, they are the ingredients you won’t find in a standard home kitchen. And the public has no idea of which UPFs are the worst hazards. Just this week, the FDA proposed banning brominated vegetable oil, found in soft drinks, previously banned in Europe and Japan, with California recently following suit, but not in effect until 2027. Recall that it took decades for the US to ban trans fats, long after this was done in Europe, despite unequivocal evidence of significant cardiovascular harm.

How many more of the countless UPF substances are toxic? As I previously reviewed, we are seeing a significant rise of cancer among young people that remains unexplained. Are UPFs, which are the dominant content of the diet in the young, contributing or even the root cause of this rise? The F in FDA stands for Food, but there is little evidence that our regulatory body has true oversight and authority about potentially toxic constituents that we’re eating. There’s not even heightened awareness of the problem led by the FDA or other public health agencies. At the very least, why haven’t food labels changed to deal with UPFs? While we’re on acronyms, it seems like this is a BFD that is being ignored.
Protein
Much of the current guidance via the National Academies’ Recommended Dietary Allowance (RDA) is based on relatively scant evidence, and is fairly similar for all people. You can get your Dietary Reference Intakes (DRI) calculated here; my US Department of Agriculture recommendations are below (vitamins and minerals are not listed). When I put in parameters for a much younger man, the output didn’t change very much, and the estimated daily caloric needs is highly influenced by your input of “active” or “very active.”
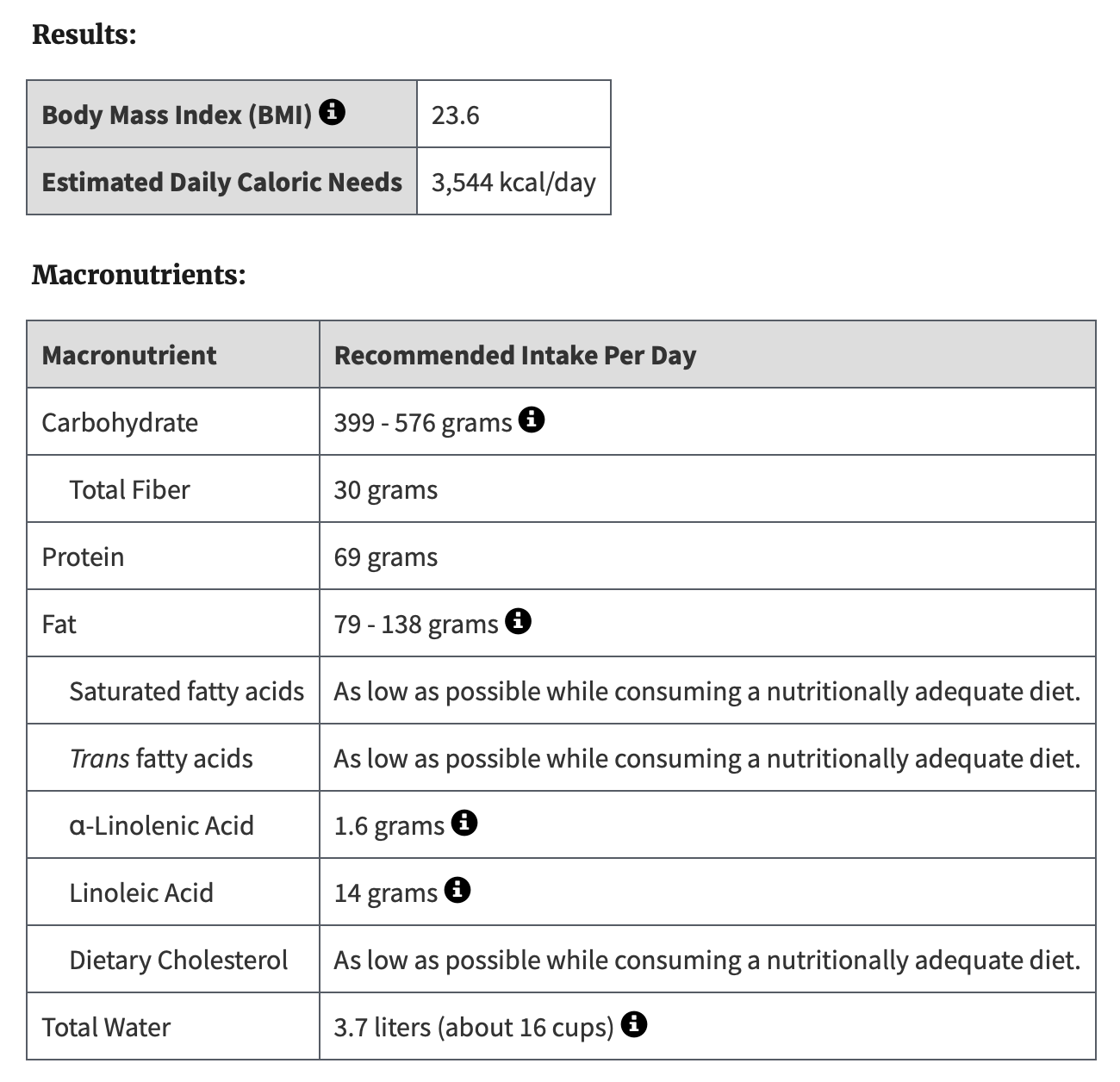
As Attia emphasized in his book, the protein RDA is remarkably low, and that will not help prevent loss of muscle mass with age —by age 80, the average person will lose 8 kg of muscle from their peak. He recommends at least twice the RDA, or about 1 gm per pound of bodyweight, an increase based on the known risk of sarcopenia—age-related loss of muscle mass and strength—that has been unequivocally demonstrated (in many studies, such as quantifying handgrip) as a risk factor for reduced healthspan. We don’t know that increasing protein in the diet with age titrates or negates that risk, which would require a randomized trial with multi-year follow up that will likely never get done. On the other hand, the risk of increasing protein in our diet, especially with aging, is minimal except in people with kidney disease. Furthermore, there’s no information on food labels about the specific amino acids (9 of the 20) in our diet that we require because we can’t synthesize, such as leucine, lysine, and methionine. Note that the DRI above breaks down fats but not proteins. With the ongoing enormous uptake of GLP-1 drugs that lead to weight loss, a significant fraction of which represents muscle mass loss, the term “sarcopenic obesity” has become a reality. And what about the people who take GLP-1 drugs, lose a lot of weight, but maintain a poor diet, rich in UPF? There’s so much we could do to upgrade our knowledge and daily awareness of protein intake that’s not being done.
A Calorie is a Calorie
Both books converge on this fundamental principle. Whereas all sorts of diets have been advocated to lose weight, it’s about the calories ingested, not principally about the ketones generated or the glycemic index.
There has been much written about caloric restriction and promoting healthspan over the years, but it’s yet unproven to promote longevity in humans. A recent publication of a small randomized trial of 75 people with Type 2 diabetes looked at time-restricted eating (TRE), calorie restriction (CR), or controls out to 6 month follow-up. As you can see in the graph below, TRE (during 8 hours in the day, between 12 N and 8 PM) fared well for weight loss, had similar results as CR for lowering HbA1c, and was found to be much easier to adhere to than calorie restriction among the study participants.
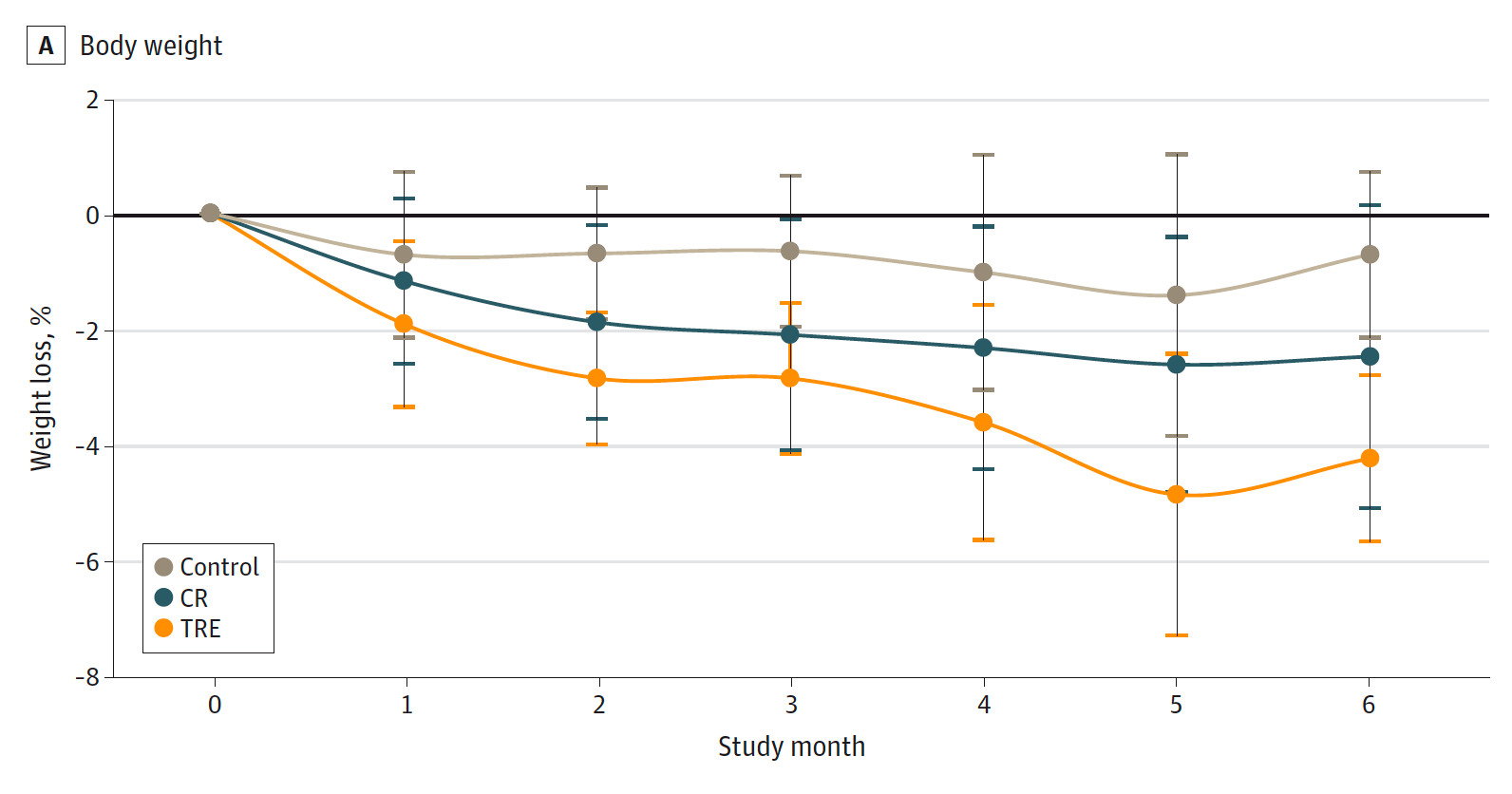
It’s clear that we take in too many calories, but practical and I daresay palatable means of reducing calorie intake need to mapped out. Rather than diets that advocate high fat or low carb, TRE may be one of the ways to achieve that irrespective of what’s being ingested. It hasn’t been adequately studied.
Please just consider this a brief summary—there’s much more that I haven’t delved into here for what we know, but a key assumption is that whatever diet is optimal will be right for all people, a premise that is likely seriously flawed.
The Future
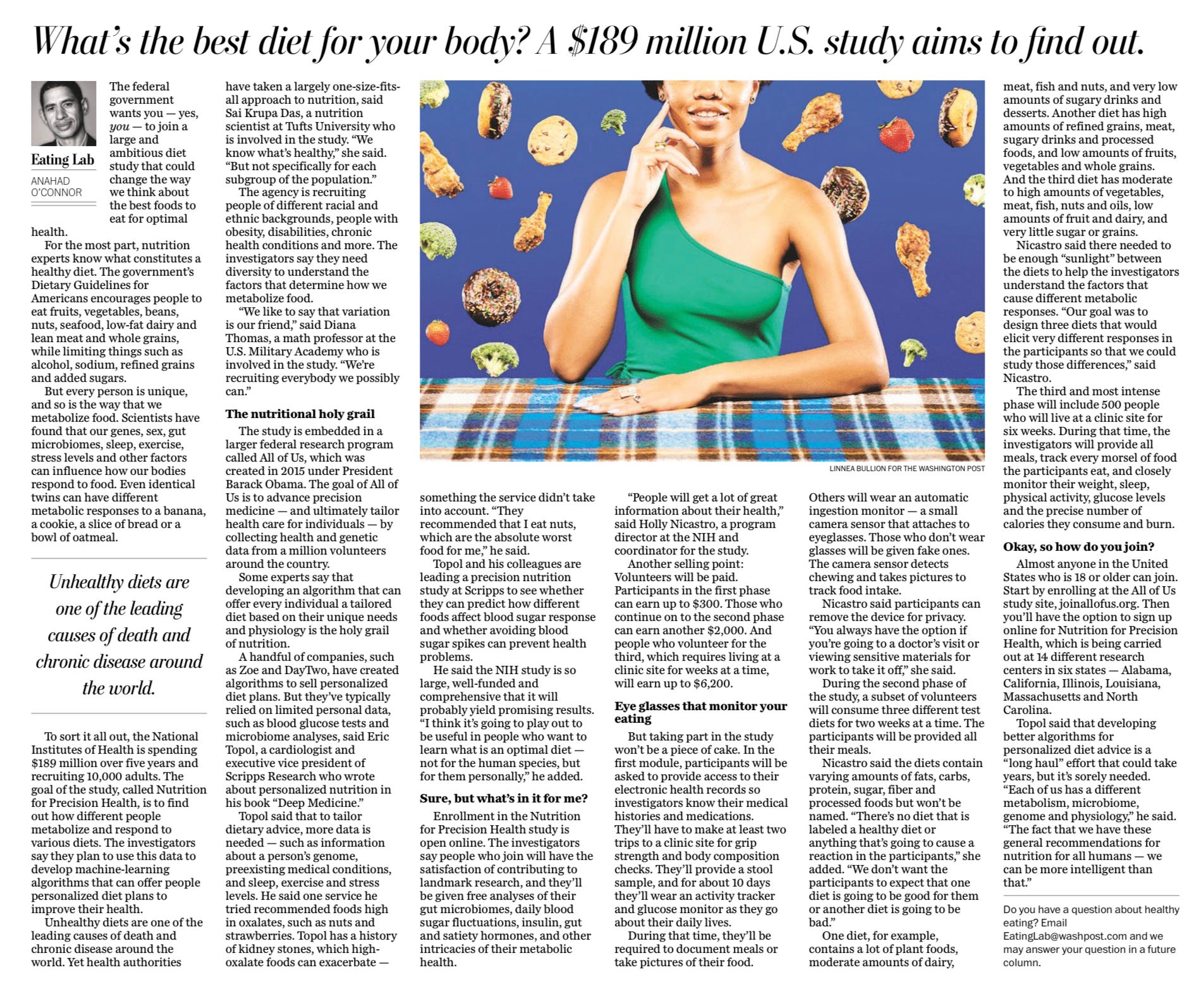
Recently, in the Washington Post, Anahad O’Connor reviewed the key aspects of the Nutrition for Precision Health NIH trial that has been enrolling since May 2023 within the All of Us Research Program. The basis for an individualized diet comes from being able to define at the granular level how unique we are with respect to our genome, our metabolome, our gut microbiome, and our physiologic make-up; how each of us responds to exercise, stress, sleep, and what we eat and drink. A classic Israeli study in 2015 that gathered multi-layered data for 800 people, highlighted the role of our gut microbiome, and laid the foundation. In 2021, the NIH announced a precision nutrition program of 10,000 American participants with “the potential to truly transform the field of nutrition science.”
The collection of all these data for each participant, which includes multiple continuous sensors, is arduous, but so is the ability to analyze the multimodal data that relies on A.I. Back in 2019, I wrote a New York Times op-ed on the concept, which the newspaper title “The A.I. Diet.” I pointed out that this is a complex undertaking, and that my first experience (using the Day Two algorithm, derived from the 2015 paper) was a bust, since the foods recommended for my optimal diet were directly contraindicated by my history of kidney stones.

The era of multimodal A.I. has just started, as I briefly reviewed in Science in September. That’s because we only now have the generative A.I. models like GPT-4 to do this work, using self-supervised (or unsupervised) learning, to integrate all of the data available for an individual, including multiple continuous biosensors along with genomic, metabolite, microbiome, electronic health record data, corpus of knowledge about foods, and everything else. Further, individualized algorithms for an optimal diet have to be validated through randomized trials—that the A.I. support versus control makes a difference and improves outcomes. It’s worth highlighting that there hasn’t yet been a report of multimodal A.I. that includes all these layers of data, particularly multiple biosensors—it’s a big analytical challenge that is bound to be cracked eventually. In the meantime, companies like Zoe are marketing personalized nutrition but there has yet to any validation that it improves health, yet carries substantial up front and monthly membership costs.
It’s very early, and certainly must be considered speculative, that we will be able to have individualized A.I. algorithms to guide each of us to an optimal diet in the years ahead. It’s also a big issue that if this endeavor is successful, will it just exacerbate health inequities that are already profound, with the people who need guidance the most the least likely to gain access?
Summary
Billionaires and venture capitalists are investing heavily in companies like Altos, Calico, Unity, BioAge and Retro Biosciences to extend longevity. It’s a big bet relying on advancing the science of aging, the embedded physiologic process that increases our risk of cardiovascular, metabolic, neurodegenerative diseases and cancer. It may ultimately pan out, as there are few domains in science that have such multiplicity of impacts on human health. Another one is nutrition. Poor diets are a key determinant of all major diseases, but optimizing nutrition gets little investment, is overly controlled by Big Food, which increasingly will use A.I. to get even better at UPFs and promoting addictive unhealthy foods. And further empowering Big Food, it’s under-regulated.
Paradoxically, nutrition isn’t something that is taught about much in medical school, but is of keen interest to the public for what is a healthy diet. We’re learning some things that can be incorporated now, but doing very little to take action. It’s great that we’re investing in a future that potentially exploits the big advances in multimodal A.I. to individualize nutrition, but that’s years away from making a difference, if it even pans out. We need to get more serious, more action oriented, and heighten awareness for what we know now. Our nutrition needs to be center stage.
Thanks for reading and subscribing to Ground Truths!
Please share this post if you found it helpful.
All content from the Ground Truths newsletter posts and podcasts are free.
Any and all voluntary financial support goes to Scripps Research.
I haven't yet finished reading this critically important post on nutrition but, I wanted to mention that I am deeply appreciative of all your writings on the Ground Truths Substack. I've been suffering from Long Covid for about a year and half now. A few weeks ago, I started working with a nutritionist towards following the Cardiometabolic Food Plan from The Institute for Functional Medicine. I have also started 5:2 intermittent fasting and am reading some of Krista Varady's research on fasting. I'm starting to lose hope regarding my recovery. I am dismayed that so many things that affect our quality of life are centered around making money. The forthright and sincere information you provide on Ground Truths gives me some hope. Thank you.
This barnstormer of a post on nutrition from Dr. Topol is a must read. Dr. Topol lays out a compelling case for investment in research and action on nutrition, starting with the eye-popping stat that a systematic study showed a poor diet is linked to 22% of all deaths worldwide.
Dr. Topol is straightforward in making the case that we aren’t doing anything like what’s needed to understand what we should and should not be eating. He notes, for example:
> “The F in FDA stands for Food, but there is little evidence that our regulatory body has true oversight and authority about potentially toxic constituents that we’re eating.”
>the “National Academies Recommended Dietary Allowance (RDA) is based on relatively scant evidence” and “the protein RDA is remarkably low, and that will not help prevent loss of muscle mass with age . . .”.
> “Poor diets are a key determinant of all major diseases, but optimizing nutrition gets little investment, is overly controlled by Big Food, which increasingly will use A.I. to get even better at UPFs and promoting addictive unhealthy foods. And further empowering Big Food, it’s under-regulated.”
As always with Dr. Topol, he doesn’t only collect and cogently explain a vast amount of information, but he also specifies what can be done to improve this sorry state of affairs. This is a clarion call, and I hope it will be read far and wide.