


A booster is your best shot now
We're heading into a new BQ.1.1 variant led wave
I know it’s hard to keep track of the new variants, with esoteric designations and without names (Hello WHO, where are you?). But several of these are quite troubling because their growth advantage compared to BA.5 (the wave we’re getting over) is substantial, chiefly related to their ability to work around our immune response.
The Major New Variants and Next US Wave
It’s been called a “variant soup” (thanks to Marc Johnson, Daniele Focosi, and Cornelius Roemer among many others, who have been tracking them closely) with so many new Omicron variants derived from the BA.2 lineage, and its BA.5 descendant. The fact that the variants converge on the same, multiple mutations (at sites R346, L452, K444, F486, N460) tell us how the virus is evolving in response to pressure of prior infection and vaccine-induced immunity. The most immune evasive variants of the whole lot are BQ.1.1 and XBB (BA.2.75.2 is not far behind). Their derivations and spike mutations (pulling diagrams together and thanks to Tom Peacock) are shown below.

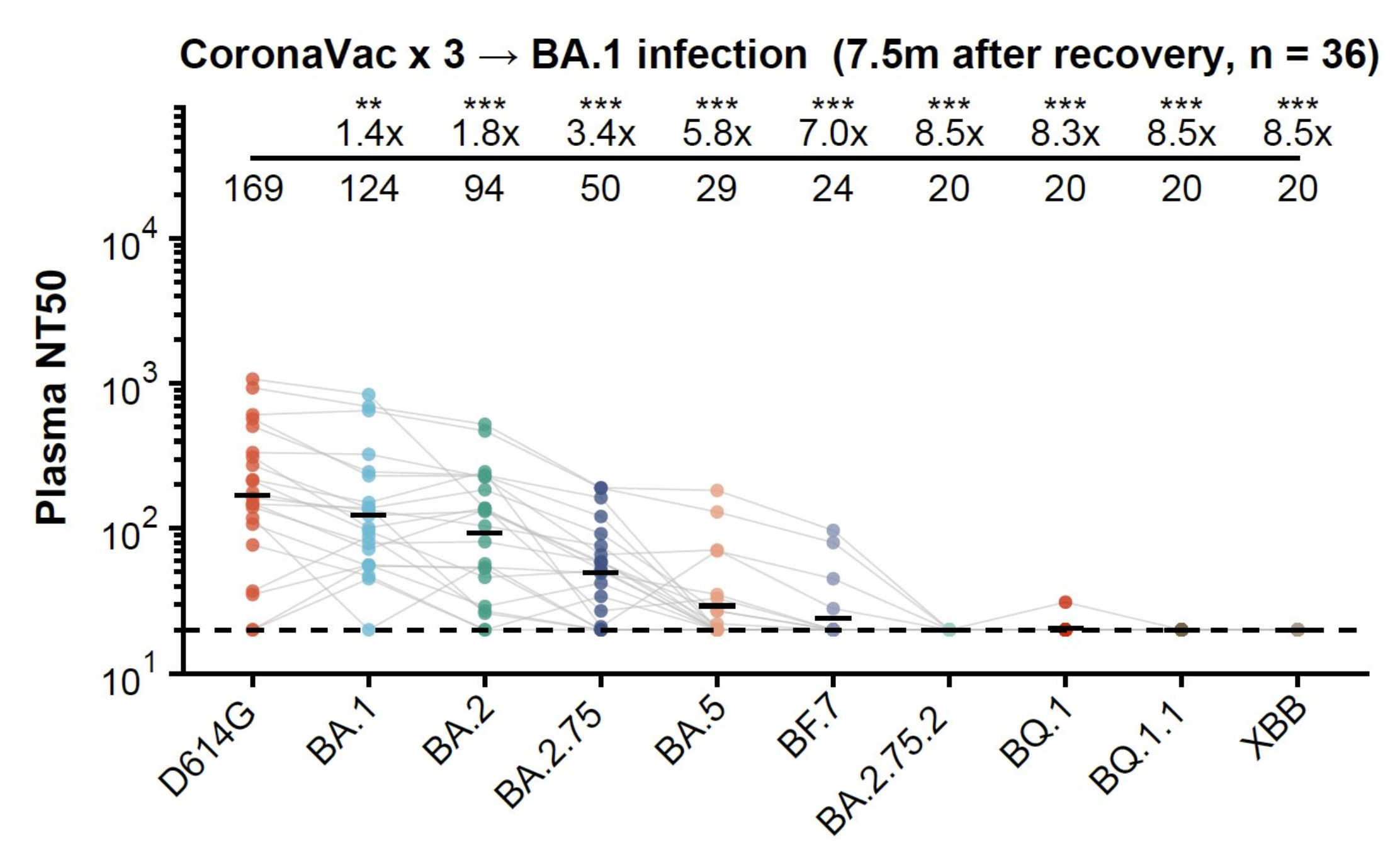
Their level of immune evasion is, in part, demonstrated by resistance to bebtelovimab, the only monoclonal antibody left that worked well against preceding versions of the virus, and Evusheld, the combination of antibodies, used for prevention by immunocompromised individuals. But the level of immune escape goes beyond that when you look at hybrid immunity —the combination of vaccines and a breakthrough infection. Yunlong Cao’s lab posted results for lack of neutralizing antibodies to BQ.1.1 and XBB (and BA.2.75.2) after 3 shots (Coronavac) and 7 months after a BA.1 infection. If anything should be considered as a red flag about immune evasion, this would be it.
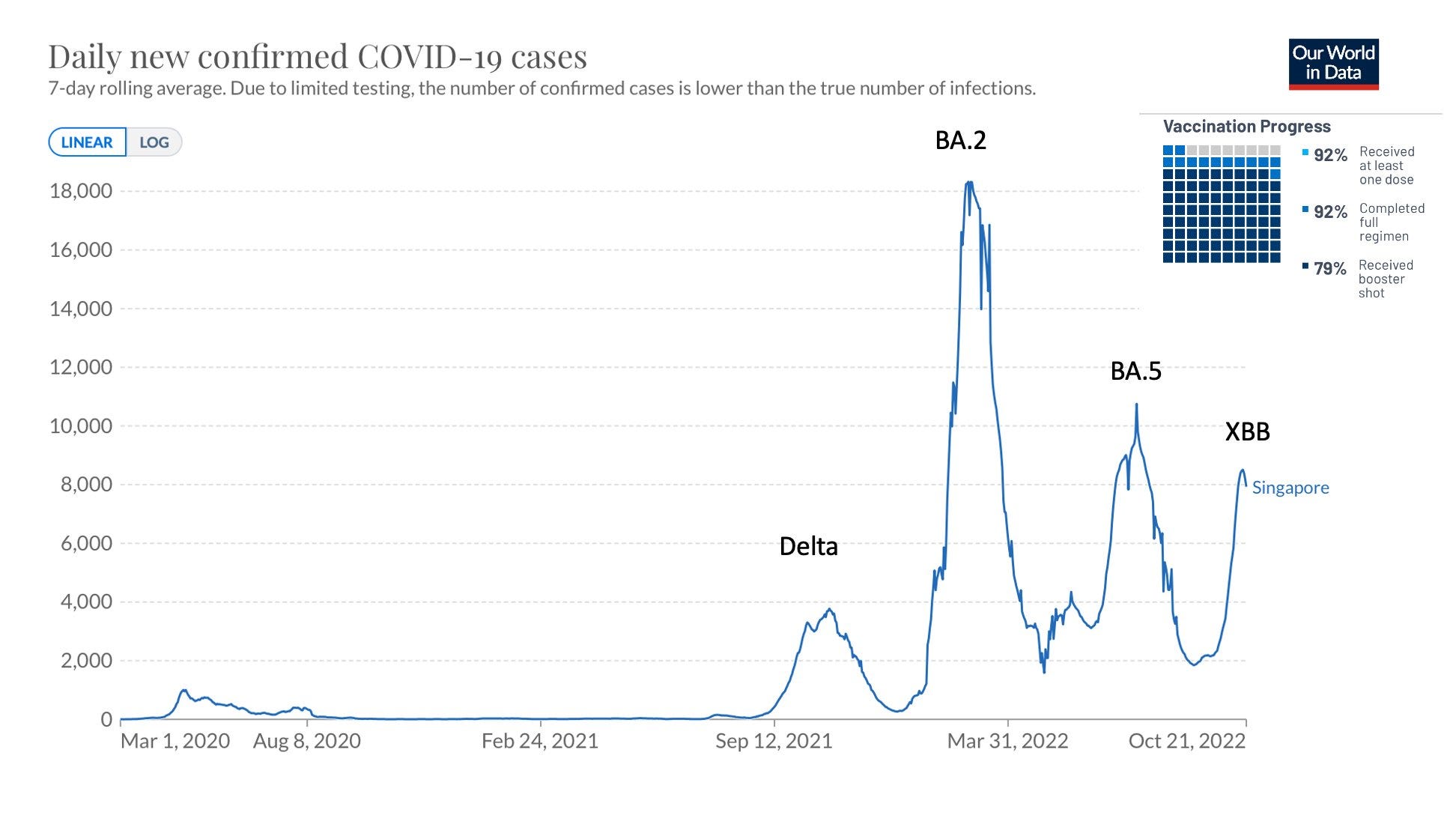
Only 1 country so far has had a new wave that can be attributed to one of these new variants—Singapore with XBB. It proved to be a significant case surge, but less than projected (expected to be worse than BA.5). That notable success, with less hospitalizations, ICU patients , and deaths than their prior 3 waves, may well be tied to the very high rate of vaccination and boosters (shown below).
In the United States and Europe the main worrisome variant that is getting legs now is not XBB, but BQ.1.1. Below is this week’s CDC report.
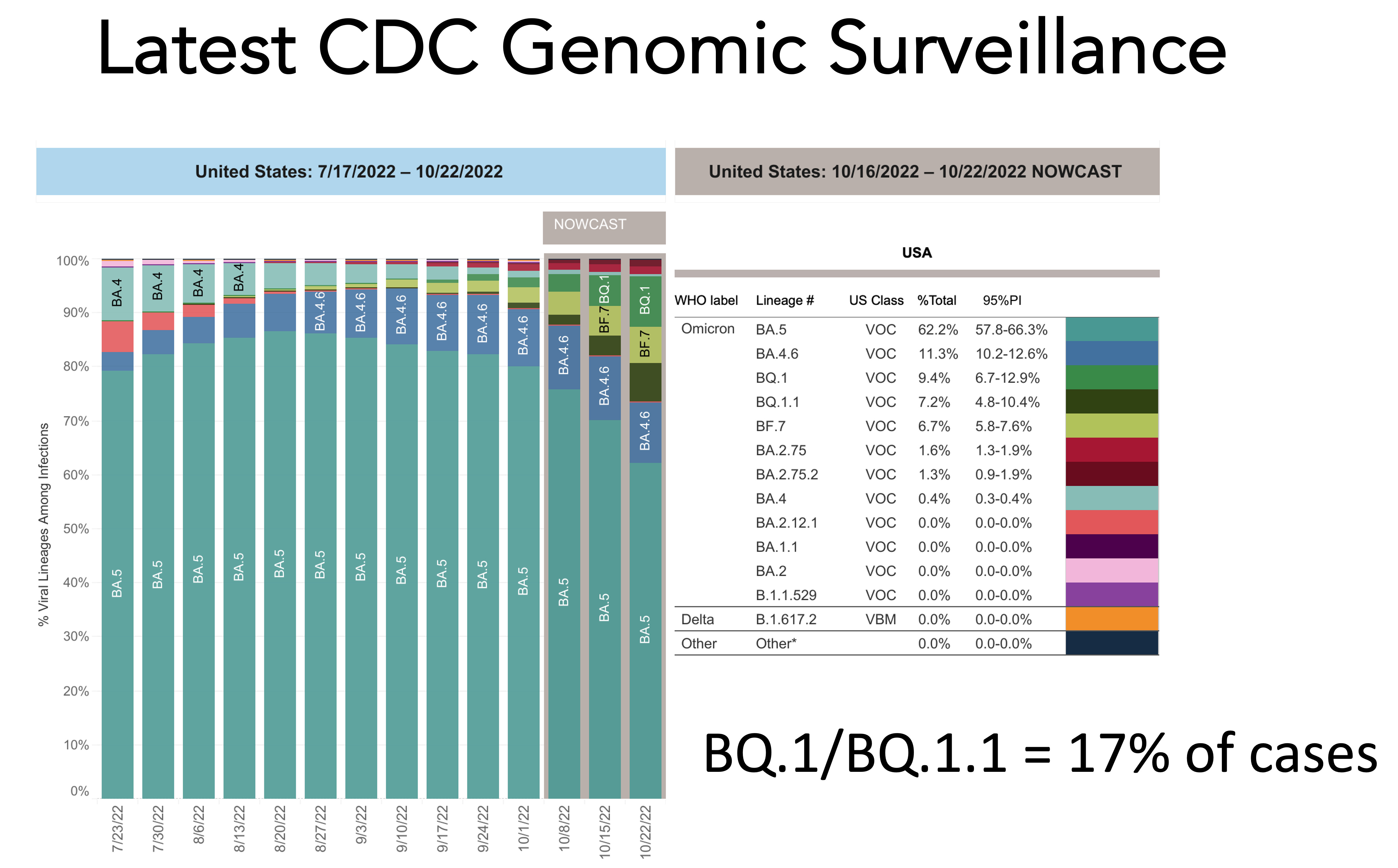
At the rate BQ.1.1 is spreading, it will reach dominance (>50%) in the next month and may, unlike prior waves with only 1 predominant variant, be admixed with BF.7 and BA.2.75.2. XBB is at very low levels in the US now, but it could rear its head later on if it can compete with BQ.1.1. (it didn’t in Singapore, but we can’t extrapolate from other countries). In New York, where there is the highest per cent of BQ.1.1 in the US, there is already a higher rate of Covid hospitalizations than had been seen since the Delta wave.
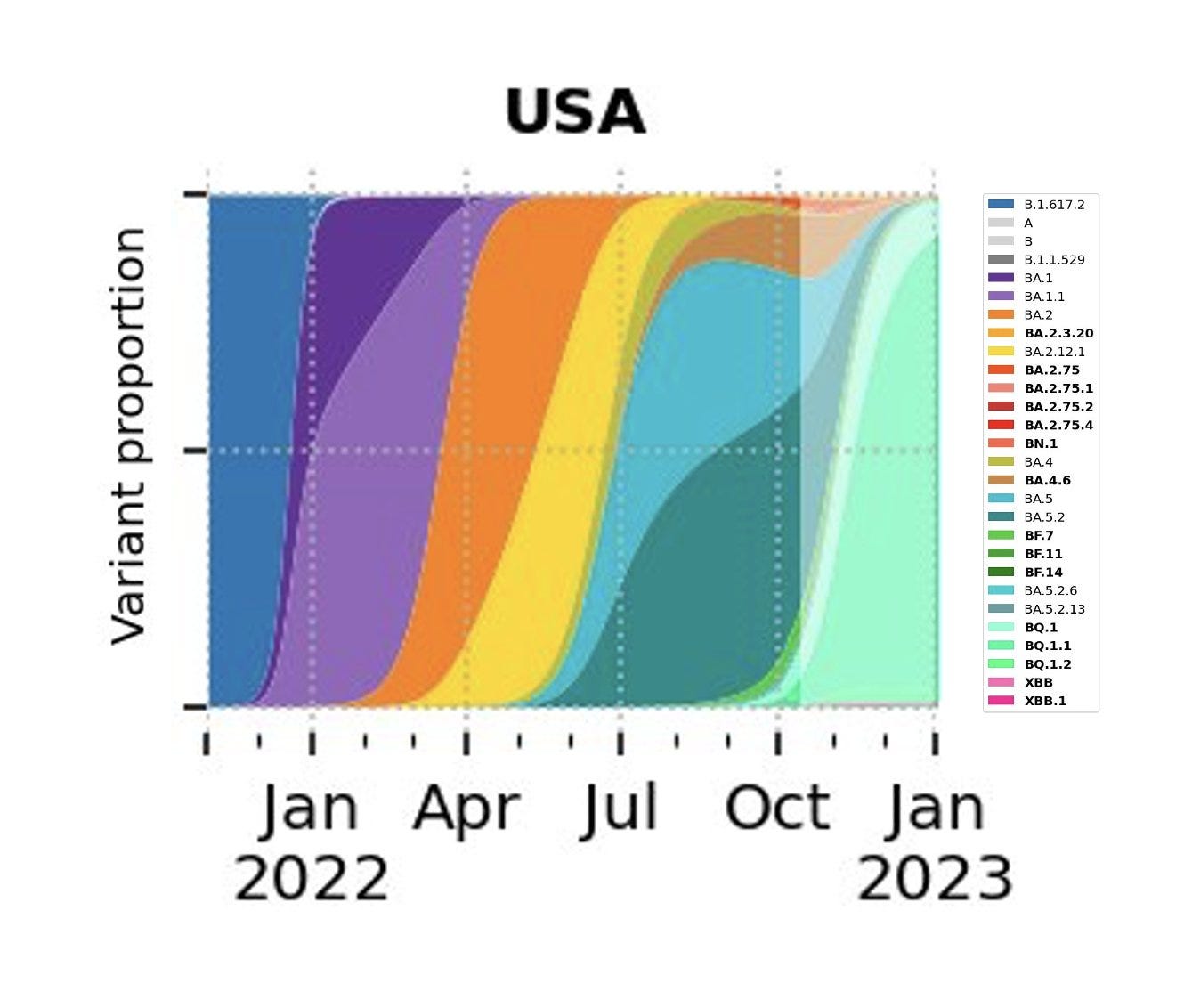
Here’s the latest projection, from Moritz Gerstung, for what the rest of the year will look like in the US, a BQ.1.x wave (←why “x”?: because BQ.1. is already picking up additional mutations, such as BQ.1.2).
The Bivalent BA.5 Boosters
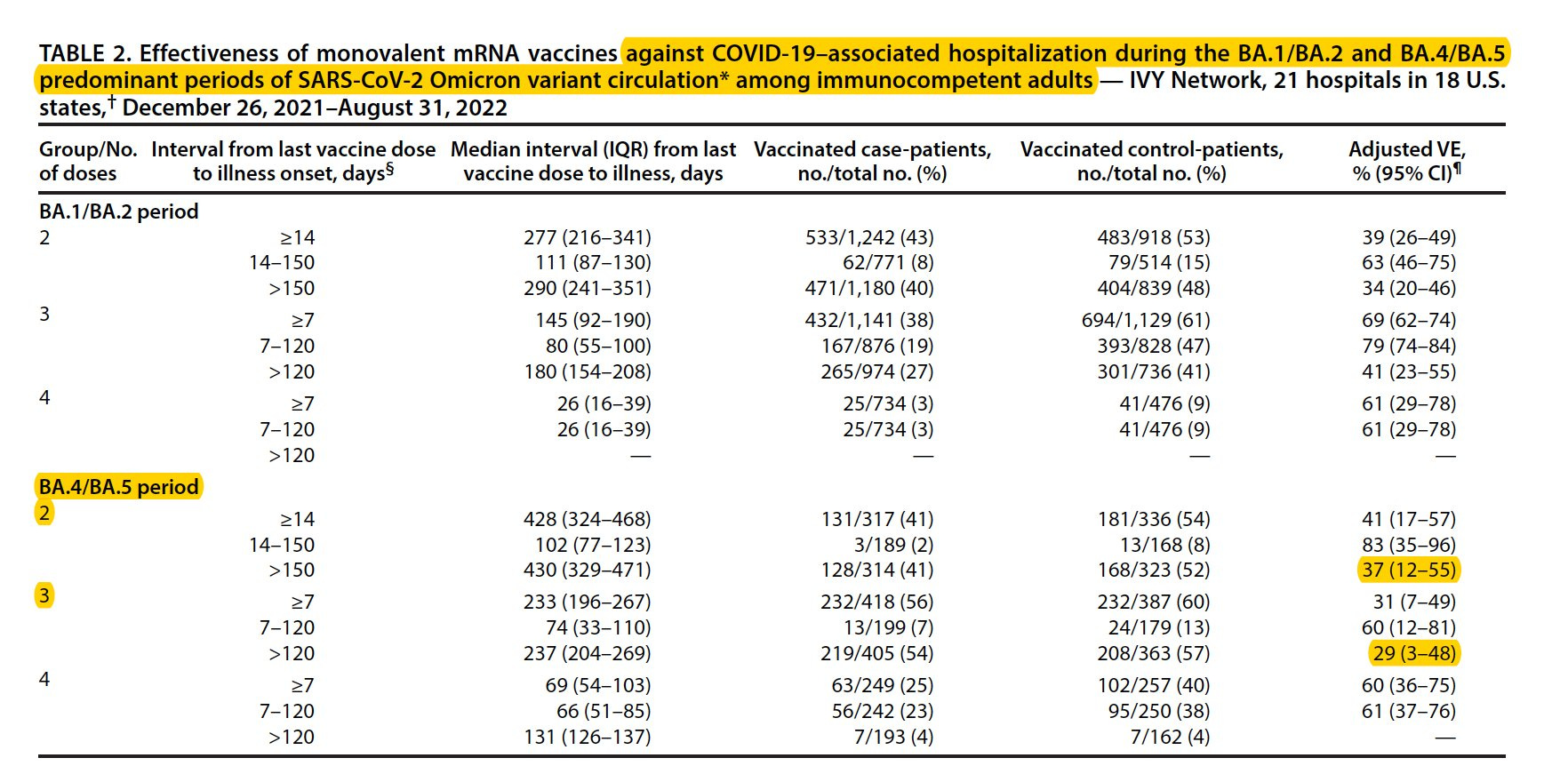
OK, so we had a rollout of a BA.5 bivalent booster vaccine that started September 2nd, for which the US purchased 171 million shots and to date, 7 weeks later, less than 12% of Americans have had one. The US is woefully under-vaccinated and under-boosted—its rate compared to Singapore and most industrialized nations for boosters is less than half. But it’s getting even worse. Every day more people are waning from vaccine-induced immunity, or infection-induced immunity, or their hybrid combination, than are getting a new booster. Our immunity wall is developing major cracks. We know waning of immunity from vaccines is substantial by 4-5 months, as reflected by a new CDC report during the BA.5 wave. Take a look at the dropdown of vaccine effectiveness after 2 or 3 shots from the report, as replicated by 2 other independent studies.
You may recall I was very critical of the BA.5 bivalent vaccine rollout, calling it a mistake, without having any human immune response data, relying only on the bivalent Beta variant small clinical trial, some BA.1 bivalent data and neutralizing antibodies from mice. Now, nearly 2 months after the BA.5 bivalent campaign started all we have is a press release from Pfizer, without any data saying there was a “substantial increase”in BA.5 neutralizing antibody response at 1 week.
……………………………………………………………………………………………………………………………
Addendum: First data on BA.5 bivalent booster in humans
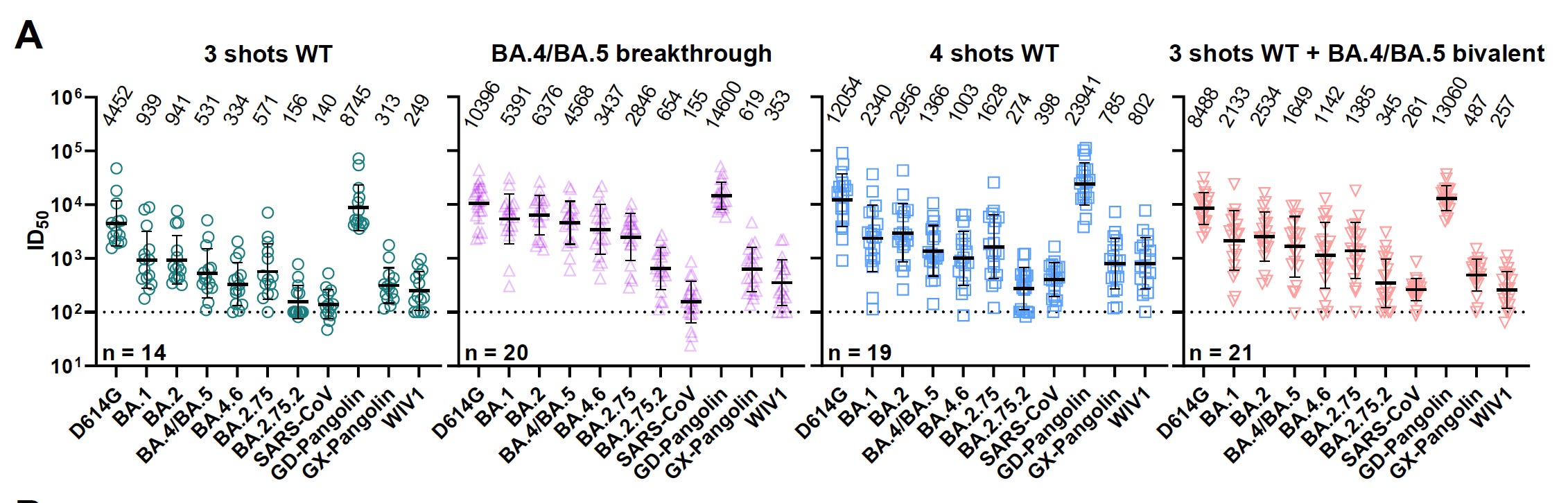
On the day following this newsletter, the highly regarded Ho lab from Columbia posted a preprint showing at 3-5 weeks, using a pseudovirus assay, there was no significant difference in the neutralizing antibody level to BA.5 compared with the original (WT, wild-type) booster. As you can see from the Figure below, 4 shots of the original vaccine compared with 3 shots of the bivalent, for each of about 20 participants (non-randomized, both Pfizer and Moderna) lacks a difference (ID50 1366 vs 1649, respectively). It is possible that later assessment will show some advantage for the bivalent, but the mice data, as I previously reviewed did not show a marked difference for the BA.5 bivalent for either the Pfizer or Moderna vaccines. It is likely this is related to an imprinting effect (see the prior links/posts) and was predicted by a report from the Nussenzweig lab:”The effects of a fourth antigenic exposure with Omicron BA.1 are limited to increased strain-specific memory with little effect on the potency or breadth of memory B cell antibodies. The results suggest that the effect of strain-specific boosting on memory B cell compartment may be limited.”
This does not detract from getting a booster, as equivalent induction of neutralizing antibodies (nAbs)—at least as good—will undoubtedly help augment the level of nAbs and broaden both humoral and cellular immunity, and improve clinical outcomes, as has been consistently seen for boosters for each of the previous major variants (Delta, Omicron BA.1, BA.2, BA.5). Undoubtedly, there will be more data forthcoming from other labs and the vaccine manufacturers on the bivalent BA.5 booster, including at later time points and with memory B cells and T cells, but this is what we have now. Although the FDA set high expectations and rushed the rollout of the bivalent without such data, the results are not surprising and should not affect any decision about getting a booster.
……………………………………………………………………………………………………………….
Nevertheless, I did go ahead with the BA.5 bivalent booster (the original was no longer available), my 3rd booster, and got marked reactogenicity with chills, fever, bad headaches, and severe fatigue lasting about 36 hours. That’s the same as I had from the 2nd, 3rd, and 4th shots. I can certainly understand why reactors like me would not want to get another booster. Unless it provided important protection.
Boosters Consistently Provide Critical, Amped Up Protection Vs Severe Covid
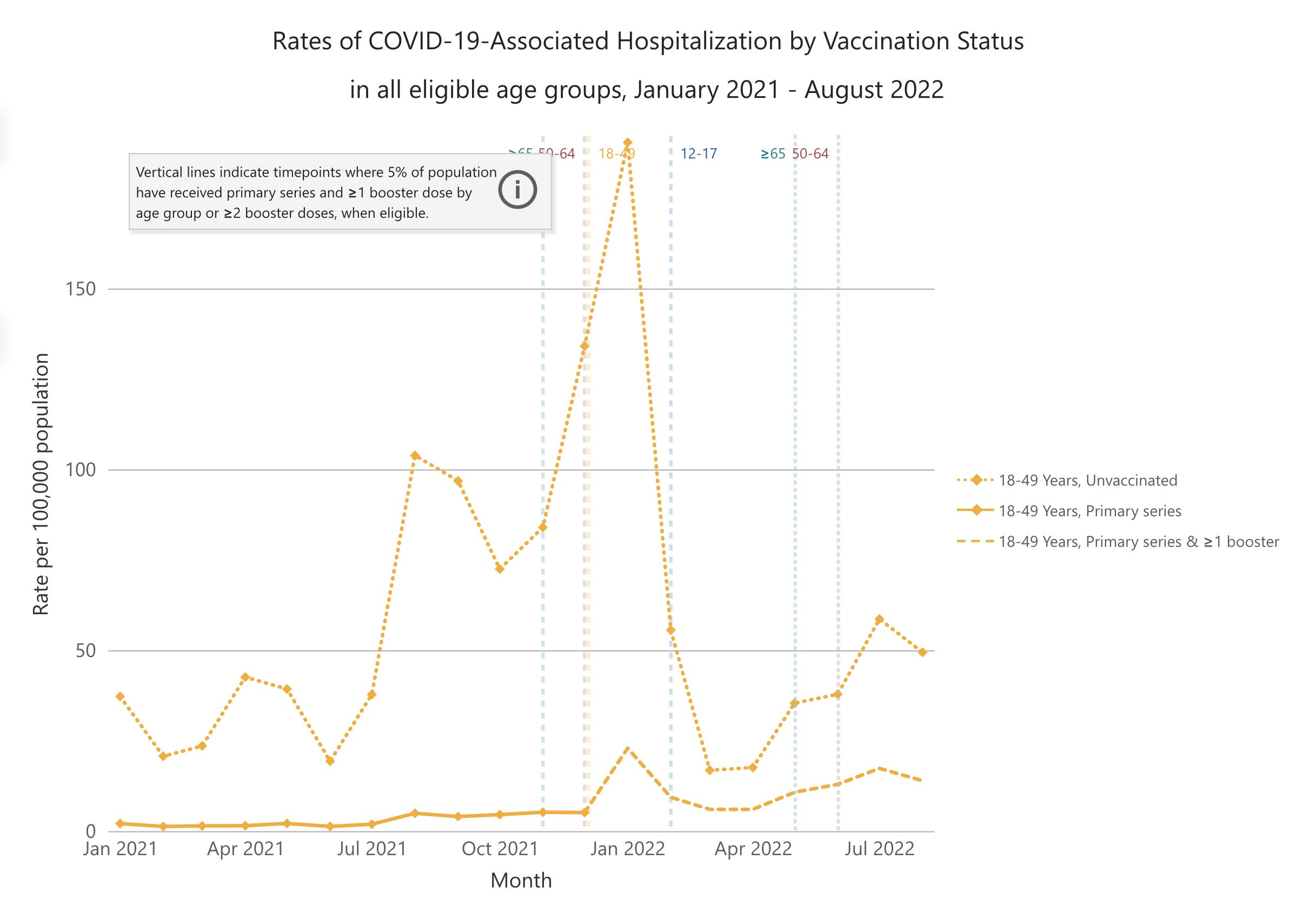
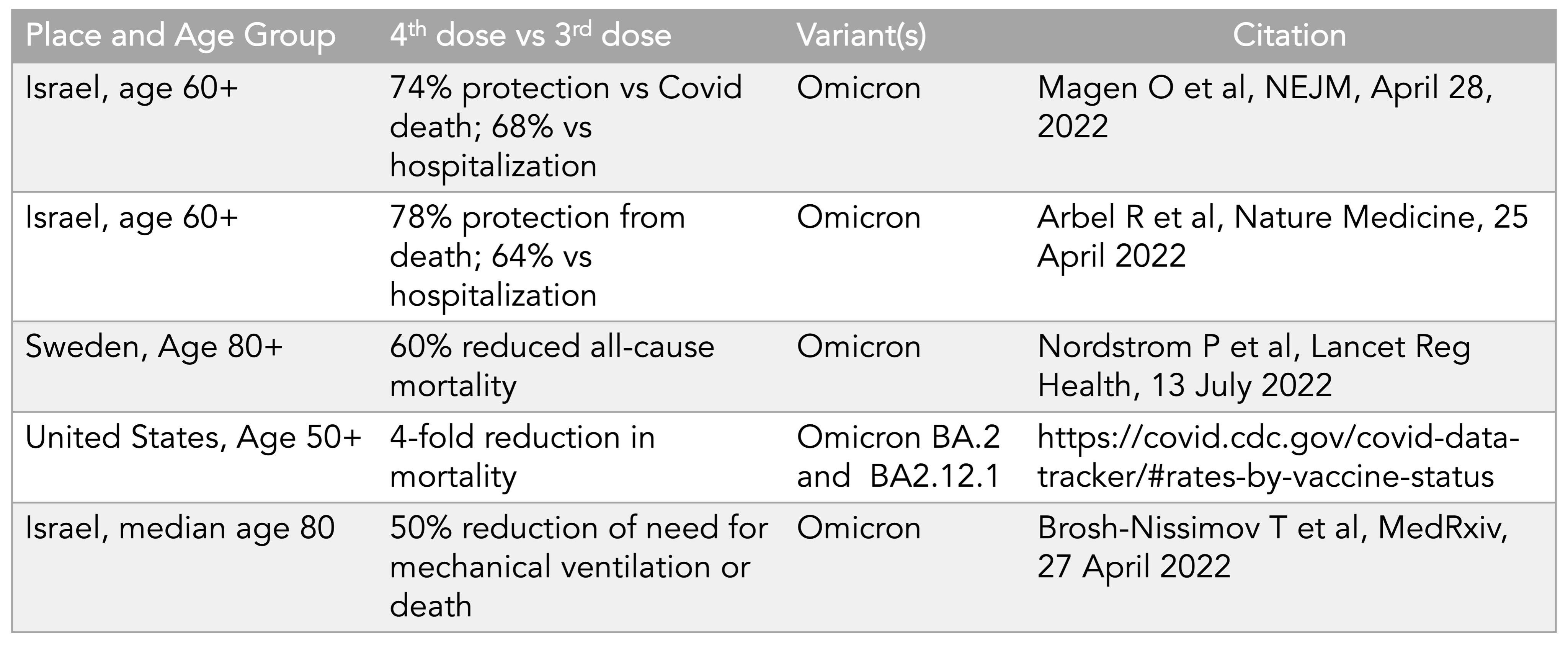
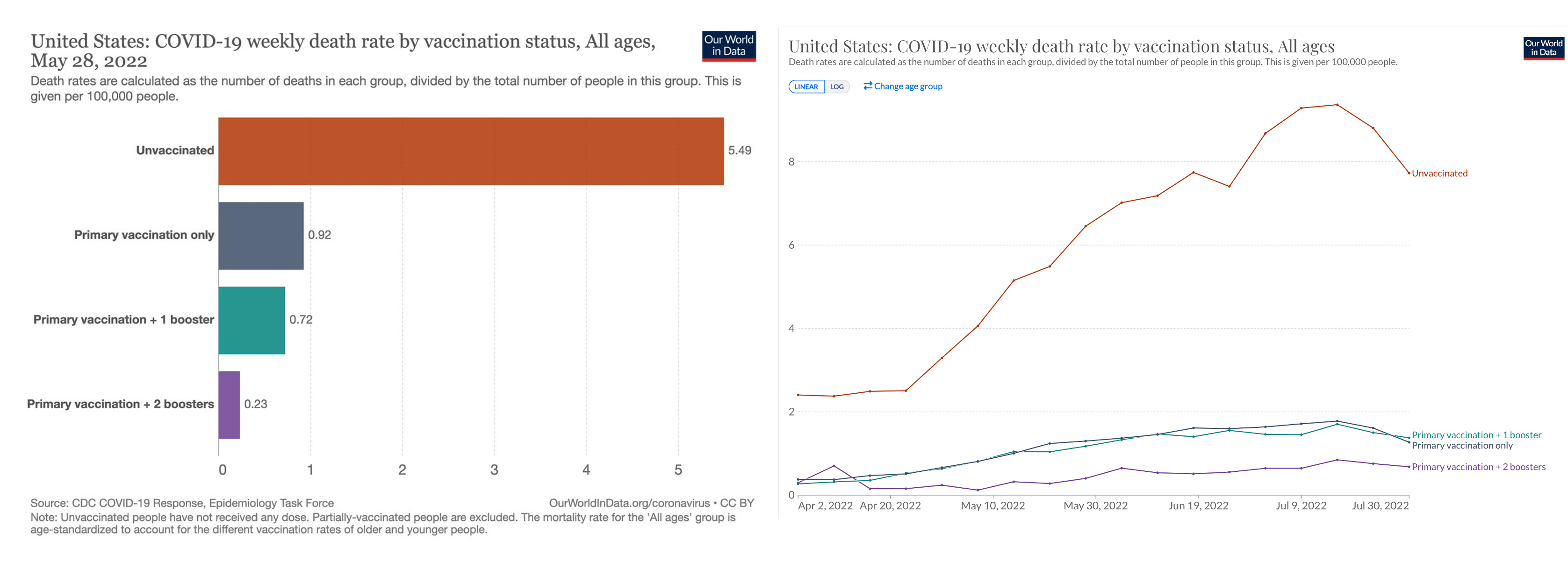
That’s what I want to review, with the premise that the new bivalent booster is at least as good as the original (ancestral) booster. We have seen more than ample recent evidence, in the US BA.5 wave that 2 boosters reduces deaths (91%) and hospitalizations for people age 50 and over, and reduces hospitalizations (72%) for people age 18-49. That body of data adds to the marked reduction death for multiple cohorts age 50 and above for a 4th shot as compared with the 3rd shot (Table below). And we know that vaccines help protect against Long Covid, by 30-50% in systematic reviews, an important benefit which should not be taken for granted.

There’s also this for 96% reduction deaths for age 18+ in May 2022, which was 91% reduction in July 2022, during the BA.5 wave, with 2 boosters compared with unvaccinated.
But with all these data reinforcing the protection from a booster, the uptake in Americans is exceptionally poor. Surprisingly, in the people who benefit the most—seniors, age 65+—the uptake is less than 10%. That leaves the highest risk population highly vulnerable with a new wave of a variant with marked immune evasion on the move. The CDC messaging has been aptly described a failure by an extensive Politico report is consistent with the US booster botch since its inception in August 2021. Why can’t the CDC present the compelling data to the public as above? The memorable statement on 60 Minutes that “the pandemic is over” by President Biden didn’t help. It’s good that he plans to have his 5th shot televised this week, but that isn’t likely to amount to a surge of new booster recipients. That we have such a big dropdown from Americans willing to have had a vaccine (79% had at least one dose) to any booster, less than 40%, provides a window to how severe the problem is and why we are ranked 73rd in countries around the world for boosters per 100 residents.
As I said to Dan Diamond is his Washington Post coverage of the poor bivalent booster uptake, “Obviously, there’s been a lot of missteps [in the government’s response]. But to me, this is the most important one: When you have people who were willing to get two shots, and then you lose them to not get a third, or a fourth, or fifth, it’s a travesty. These are people who are willing to get vaccinated.”
Yes, there are disappointing features about boosters that arose with arrival of the Omicron variant in 2021 (and subsequently its descendants). That mutation-laden new family of variants is what’s responsible for the “leaky” feature of vaccines which, through the Delta variant wave, with a booster were 95% protective against infections and there was a <1% rate of reinfection. Boosters will not have a substantial or durable impact for preventing infections or transmission. That’s why the use of high-quality masks, ventilation, air filtration, and the known mitigation factors, still play a role in the right settings. We already know that from multiple reports of BA.5 breakthroughs, in people who had a recent bivalent BA.5 vaccine, as we’ve seen this weekend with our CDC Director (hope for a rapid and complete recovery for Dr. Walensky). And we can’t, at a population level, be getting boosters every 4-5 months to maintain protection against severe Covid, especially knowing the proportion of people unwilling keeps increasing with each waning period. The idea that we could be looking annual shots is unrealistic given the waning period and lack of clearcut seasonal Covid as is the case with flu. That is why we desperately need new generation of vaccines that include nasal vaccines to block infections/transmission, more durable vaccines (such as by tweaking the nanoparticles) and pan-sarbecovirus vaccines that will be variant-proof. All of this is in our reach, but so far not getting the priority and resource allocation from the US to follow through.
For now, the best defense we have against the BQ.1.1-led wave is to get a booster. It will markedly raise neutralizing antibodies and our cellular immune response, and just-in-time to broaden our immunity to be ready for BQ.1.1 and related variants with marked immune evasiveness. As you well know, it takes a couple of weeks to get the immune response built, so this is the right time to get it done. It will help prevent severe Covid for at least 4-5 months ahead. Be ready. The pandemic isn’t over—yet. Preserve your health and that of your family, friends, and network.
Thanks for reading. Subscriptions to Ground Truths are free, and always will be.